---
Publish Now: null
author:
- Yujan Shrestha
cta_button_text: Supercharge your FDA timelines
cta_case_studies:
- 35cbd5b7-a754-80f4-9a3c-cc0e62e41d52
- 30abd5b7-a754-8063-90d4-ea45a37122f6
- a4b2d790-f1ff-47bb-93b2-09b0d4619030
- 141bd5b7-a754-80c4-8e9a-fa24807a2e59
cta_hero_details: 'The new deal pays out in interaction speed: 45-day follow-up pre-subs,
same-week informal answers, a de novo goal you can finally put in a board deck.
Extracting that speed takes scoped questions, complete submissions, and AI/SaMD
fluency your review team will test. Innolitics has cleared 50+ SaMD products, with
AI submissions delivered in as little as 3 months. Bring us your pipeline and we\''ll
show you where the new machinery cuts months off it.'
cta_hero_text: MDUFA VI rewards the teams that iterate fastest with FDA. Is yours
built for it?
date: '2026-07-08'
description: FDA\'s draft MDUFA VI commitment letter (FY2028--2032) restructures how
sponsors interact with the agency. Seven changes that will reshape submission planning
for software and AI device teams, plus a side-by-side comparison with the current
MDUFA V deal (including the quietly reset 510(k) clock), with highlighted evidence
from both documents.
related: []
title: 'MDUFA VI vs. MDUFA V: The Side-by-Side Every Regulatory Lead Should Read'
topics:
- Regulatory
- AI/ML
- News
---
*FDA\'s draft commitment letter for FY2028--2032 rewrites the mechanics of how sponsors interact with the agency. Here\'s what changes if you\'re building software as a medical device, and what to adjust in your regulatory strategy now.*
Every five years, FDA and the medical device industry negotiate the Medical Device User Fee Amendments (MDUFA): the deal that sets FDA\'s review performance goals in exchange for industry user fees. The draft MDUFA VI commitment letter, covering fiscal years 2028 through 2032, was released in June 2026.
Most coverage will focus on the headline review timelines. The more consequential changes are structural: FDA is rebuilding how sponsors talk to reviewers, converting its deficiency-letter quality bar from a five-year ramp into a permanent audited floor, and, for the first time in a MDUFA letter, naming generative and agentic AI as areas it will staff and build review policy around.
I read the full 36-page draft. Here are the seven changes that will reshape how software and AI device teams plan submissions, and what to do about each.
Source: draft MDUFA VI commitment letter, p. 3 — shared FDA/industry
responsibility and the 285-day PMA shared outcome goal (highlighted).
### Every timeline change at a glance
Before the analysis, the numbers. The honest summary for planning purposes: FDA is committing to faster conversations and more predictable decisions, not faster total review clocks. The interaction goals (pre-subs, de novo certainty, escalation rights) genuinely improved. The end-to-end review goals held flat or reset. Here is every timeline that moved, held, or vanished:
| What\'s timed | MDUFA V (current deal) | Draft MDUFA VI (FY2028--2032) | What it means for you |
|---------------------------------------------------------------|---------------------------------------------------------------------------|----------------------------------------------------------------------------------|--------------------------------------------------------------------------------------------------------------|
| Follow-up regulatory questions | 70-day written feedback (a full pre-sub each time) | **45 days** via the new Focused Follow-Up Pre-Sub | The biggest genuine speedup: each strategy iteration with FDA gets about a month shorter |
| Quick questions (single reviewer, \~30-minute scope) | No tracked channel | Answered outside the pre-sub process; tracked portal mechanism by September 2029 | Same-week answers for narrow questions instead of a 70-day round trip |
| Traditional pre-sub written feedback | 70 days for 90% | 70 days for 90%, up to 5,000 per year | Unchanged, but pre-subs gain a fee (credited back on a later marketing submission) |
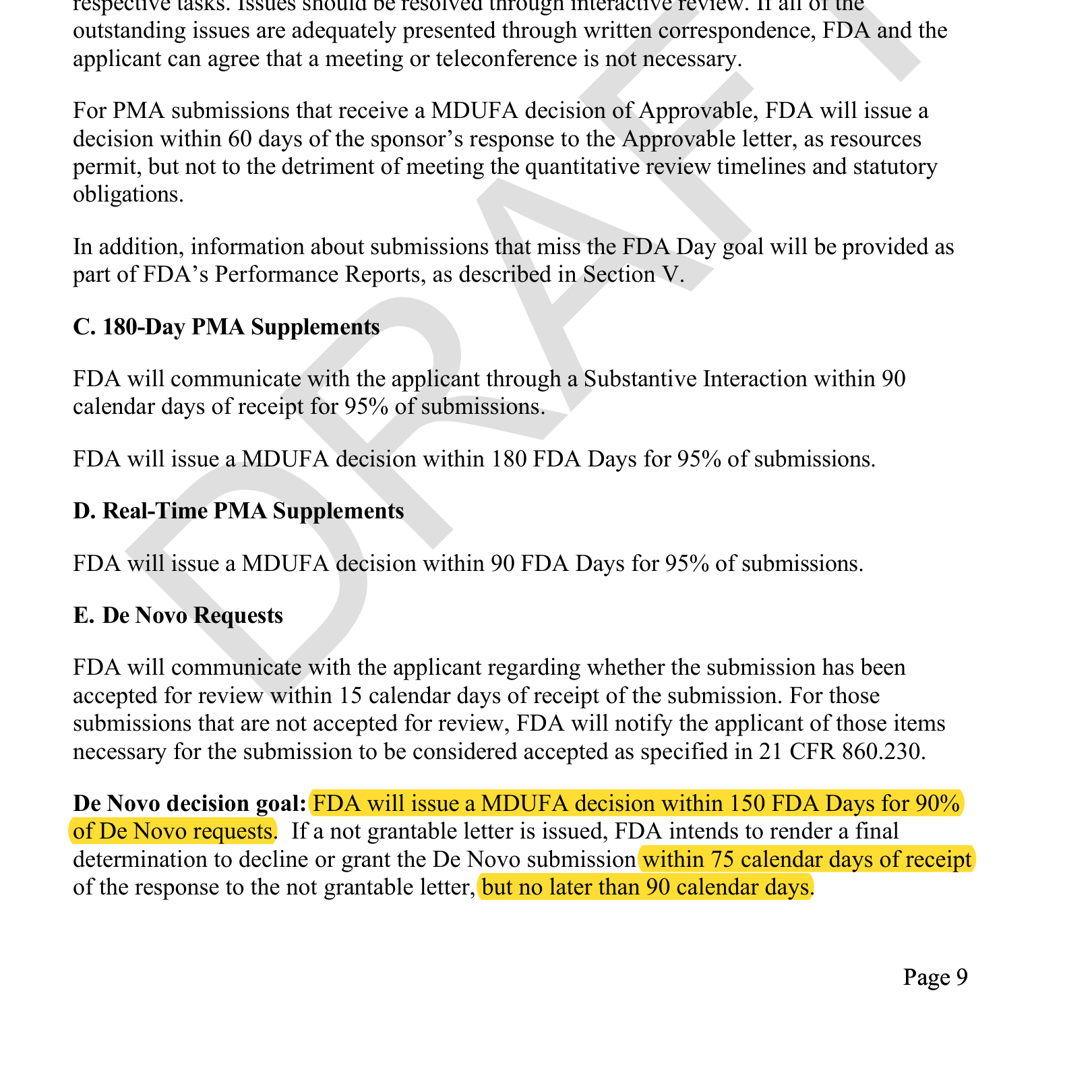
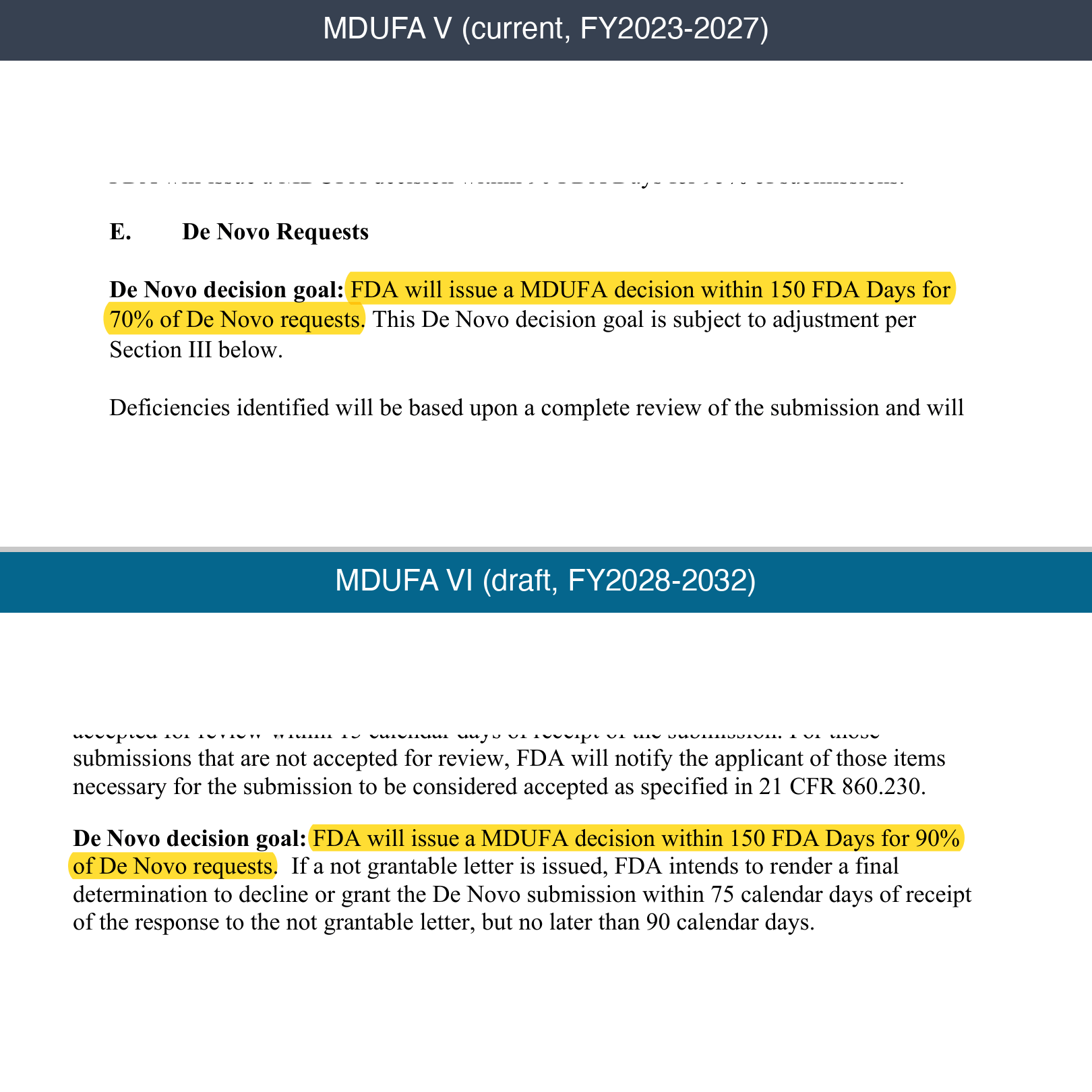
| De novo decision | 150 FDA days for 70% of requests (90% only as a conditional stretch goal) | 150 FDA days for **90%**, guaranteed from day one | Same clock, but now reliable enough for a board deck: pathway risk drops sharply |
| De novo kickoff | No early meeting | Introduction Meeting within the first 30 FDA days | You align with the review team at the start, not after the first deficiency letter |
| De novo \"not grantable\" resolution | No goal | Final determination within 75--90 calendar days of your response | Ends the open-ended limbo after a negative letter |
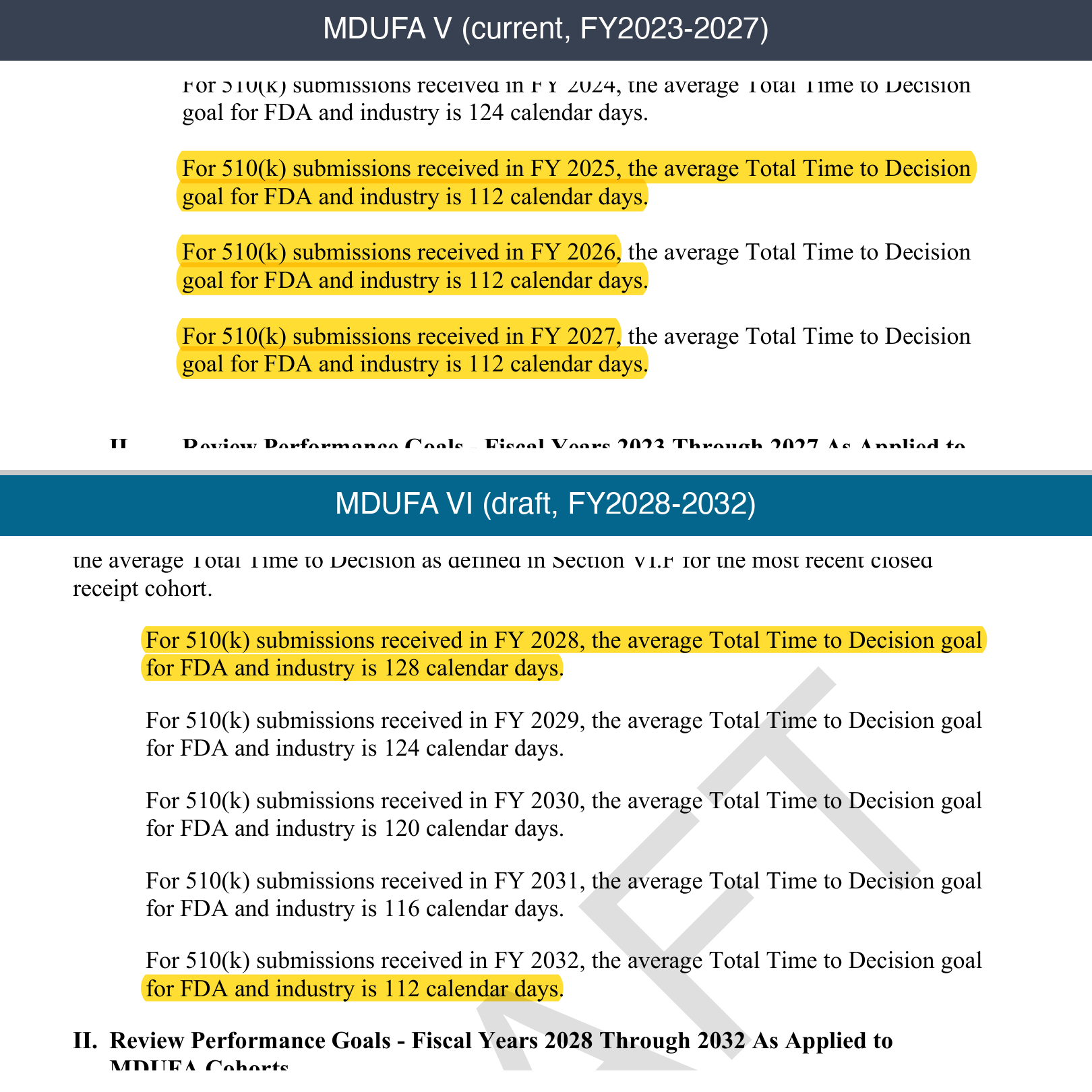
| 510(k) total time to decision (FDA + industry days) | 128 days (FY2023) stepping to 112 by FY2025 | 128 days (FY2028) stepping to 112 by FY2032 | **Not faster.** The ladder restarts where 2023 did; model \~4 months of review calendar, not the finish line |
| 510(k) FDA decision goal | 90 FDA days for 95% | Unchanged | The core 510(k) review clock holds steady |
| 510(k) stalled past 100 FDA days | Written feedback plus a meeting with action items | Carried over | A built-in escalation checkpoint most sponsors never use |
| PMA (original and panel-track) total time | 290 days, then 285 from FY2025 | 285 days flat through FY2032 | No committed improvement |
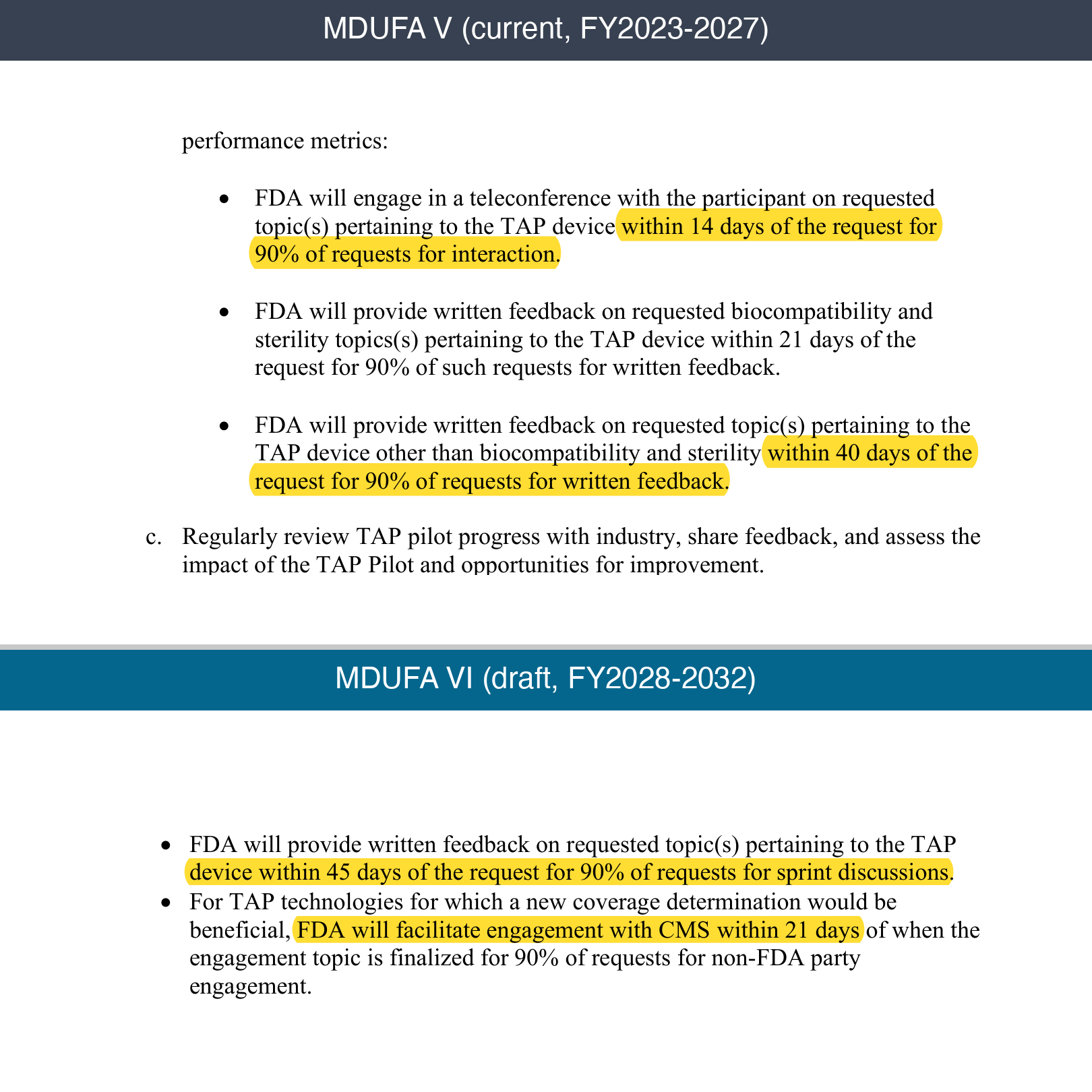
| Breakthrough/TAP teleconference | 14 days (pilot) | 21 days (full program, all OHTs) | Slightly looser, in exchange for program-wide access |
| TAP written sprint feedback | 40 days (21 for biocompatibility/sterility) | 45 days | Slightly looser |
| TAP reimbursement (CMS) engagement | Did not exist | FDA facilitates CMS engagement within 21 days of finalizing the topic | New, and commercially the biggest: coverage strategy starts before clearance |
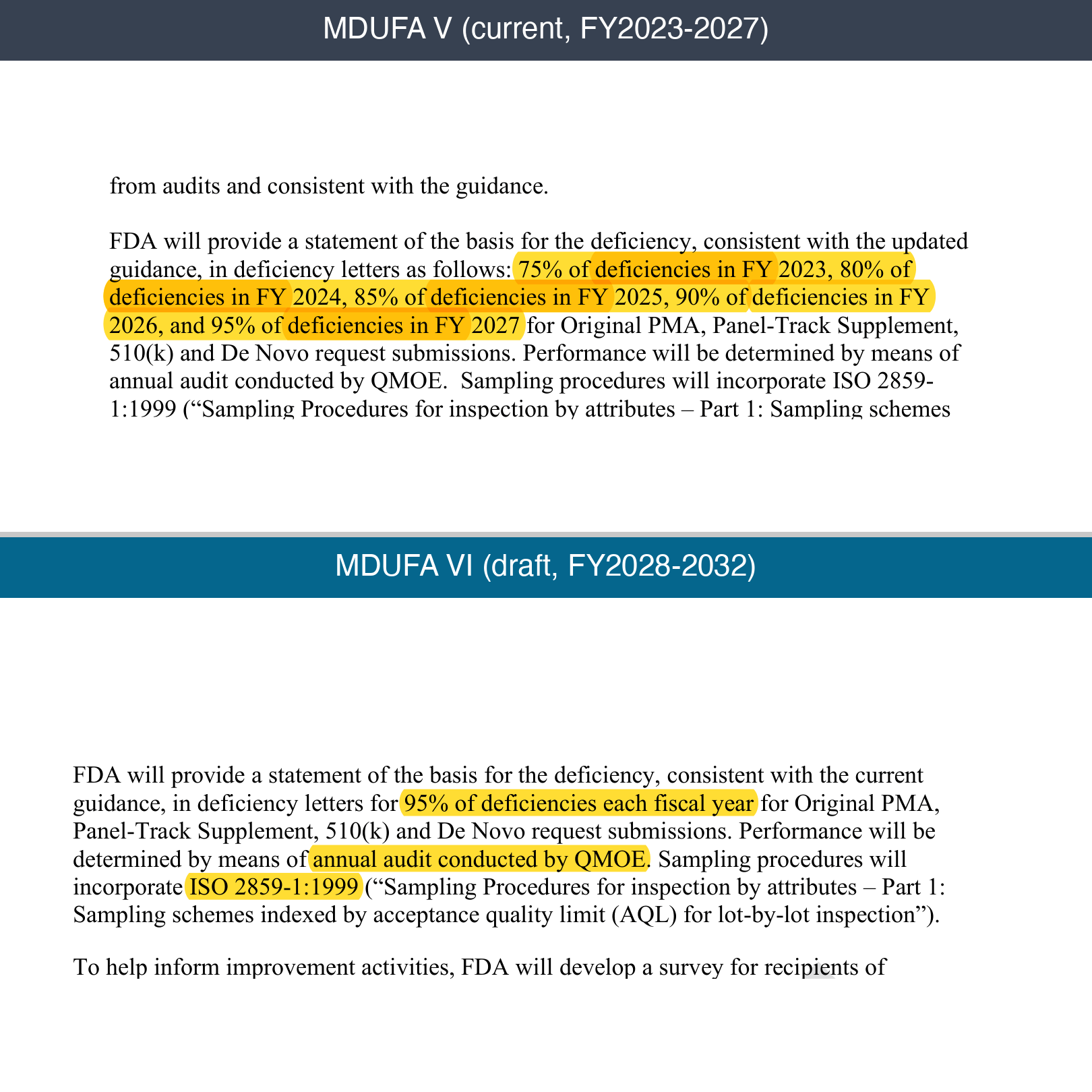
| Deficiency letters with stated basis | Ramp: 75% (FY2023) to 95% (FY2027) | 95% every year, independently audited | Fewer surprise deficiencies, and standing to push back when one arrives unexplained |
| Stretch goals (108-day 510(k), 270--275-day PMA, 90% de novo) | Available if triggers were hit | Deleted | The printed numbers are the ceiling; build plans with no upside scenario |
*Numbers verified against the* [*MDUFA V commitment letter*](https://www.fda.gov/media/158308/download) *and FDA\'s* [*Federal Register summary*](https://www.federalregister.gov/documents/2026/07/08/2026-13778/medical-device-user-fee-amendments-public-meeting-request-for-comments) *of the draft MDUFA VI letter (July 8, 2026).*
### 1. Pre-submissions become iterative: the Focused Follow-Up Pre-Sub
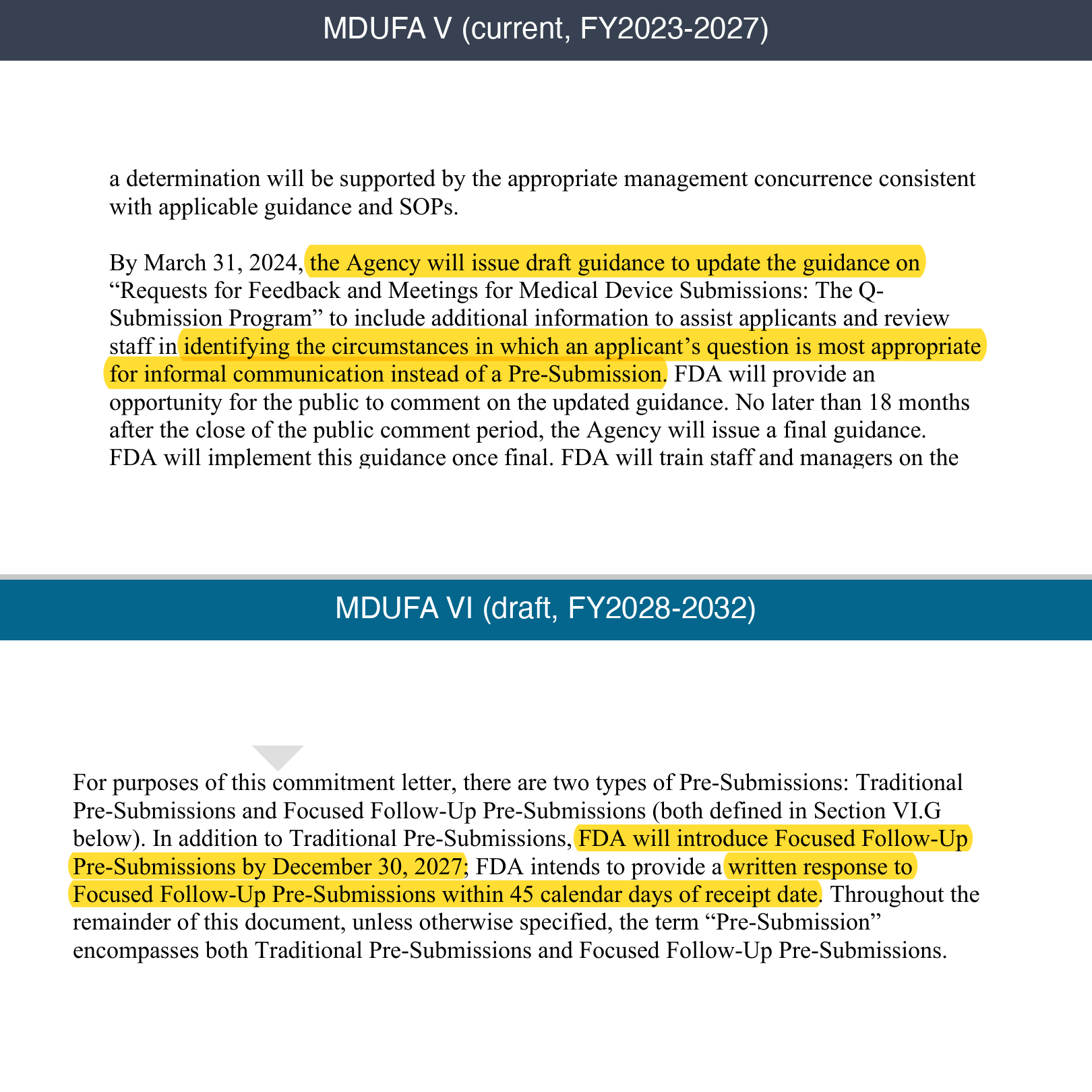
The single biggest practice change. Starting by December 30, 2027, FDA introduces a new submission type: the Focused Follow-Up Pre-Submission.
- Written FDA response within **45 calendar days** (versus the \~70-day goal for traditional pre-subs).
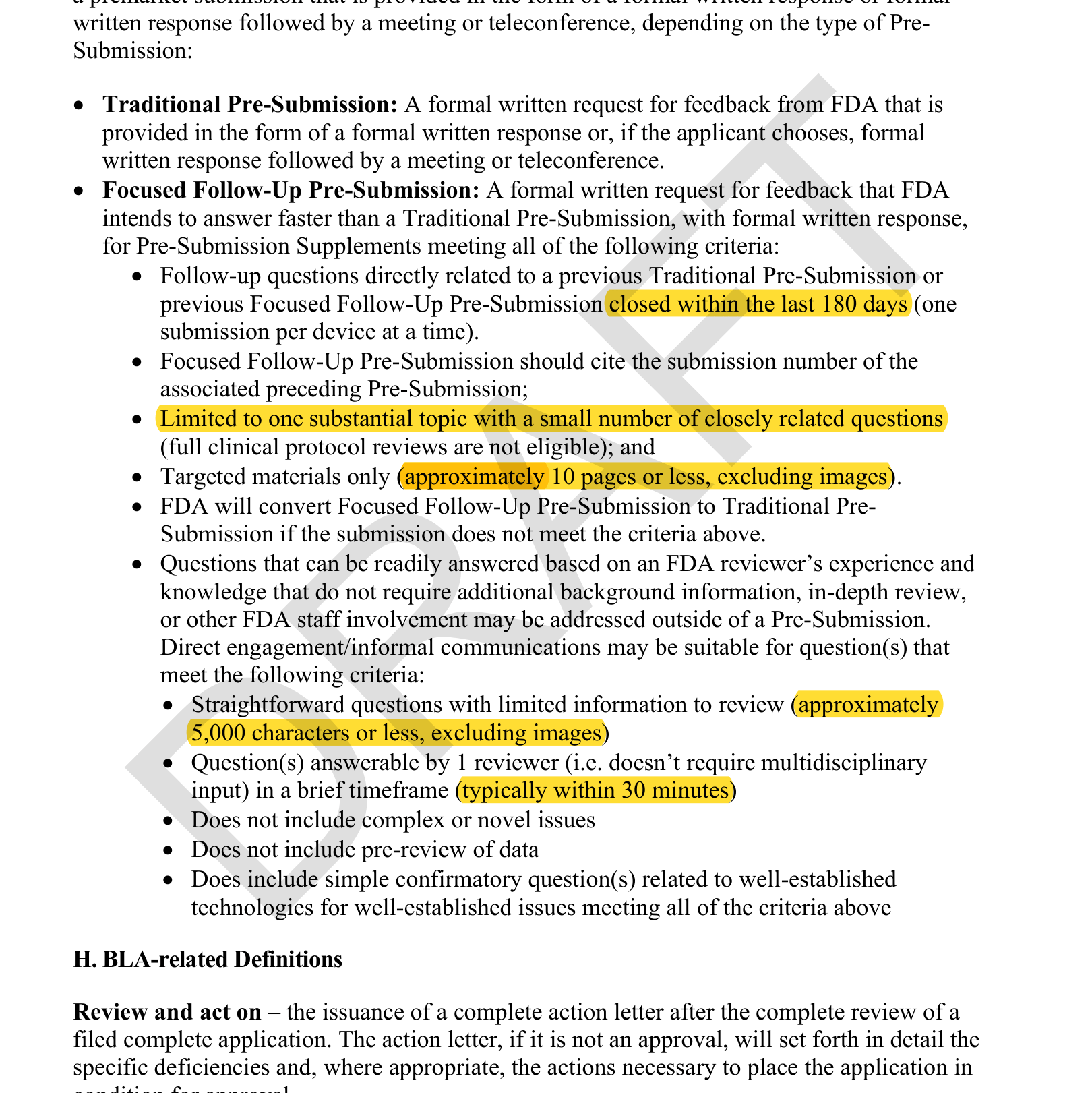
- Eligible when your questions follow directly from a pre-sub closed within the last 180 days.
- Limited to one substantial topic, a small number of closely related questions, and roughly 10 pages of targeted material. Full clinical protocol reviews are not eligible.
Alongside it, FDA is formalizing a direct informal communication channel: questions under \~5,000 characters that a single reviewer can answer in about 30 minutes (no complex or novel issues, no data pre-review) can be answered outside the pre-sub process entirely, eventually through a tracked mechanism in the Customer Collaboration Portal (committed for September 2029).
**And the trade nobody\'s headlining: pre-submissions stop being free.** The commitment letter doesn\'t say it --- the statutory package negotiated alongside it does. FDA and industry agreed to propose a new FD&C Act fee for initial Pre-Submissions, explicitly \"to encourage more strategic and thoughtful utilization of the program.\" The mechanics soften it: a flat fee on the original pre-sub only --- supplements, Focused Follow-Ups, and informational Q-subs stay free --- and the fee functions as a credit toward your subsequent marketing submission fee when you file. Breakthrough- and STeP-designated devices are exempt. (Fee amounts will be set in the annual fee notices; none published yet.)
Source: Federal Register, July 8, 2026 (Doc. 2026-13778), MDUFA
reauthorization public meeting notice — "FDA and industry agreed to
proposed changes to the FD&C Act to include a fee for initial
Pre-Submissions... for which sponsors will later receive a corresponding
credit on certain related subsequent marketing submission fees"
(highlighted). This change is in the statutory package, not the draft
commitment letter.
**What to do:** Stop writing pre-subs like dissertations. The sponsors who win under this system will sequence their regulatory questions like an engineering backlog --- one scoped decision at a time, each follow-up building on a documented prior answer. Batch-everything pre-subs were already a weak strategy; now the fee structure enforces the iteration model: you pay once for a well-scoped original, then iterate free through Focused Follow-Ups and informal questions.
And note the failure mode. Or rather, the lack of one. If FDA decides your Focused Follow-Up doesn\'t qualify, it doesn\'t get rejected; it gets converted to a Traditional pre-sub, with FDA telling you which criteria you missed and offering meeting dates. That makes the fast lane a free option: try it whenever you\'re close to eligible, because the downside is the process you\'d have used anyway. (Same logic as attempting a Special 510(k): if FDA declines, they just convert it to Traditional.)
Two caveats. First, the Focused Follow-Up lane is written-only: when a dispute turns on statistics, you still want a Traditional pre-sub meeting, and if FDA is bringing a statistician, bring yours; those calls turn entirely on the statistics. Second, these channels are worth exactly as much as their proximity to your actual review team. Feedback from staff who won\'t be reviewing your submission, however fast, is optics, not signal.
Source: draft MDUFA VI commitment letter, p. 4 — Focused Follow-Up
Pre-Submissions introduced by December 30, 2027 with written response
within 45 calendar days (highlighted).
Source: draft MDUFA VI commitment letter, p. 35 — Focused Follow-Up
eligibility (prior pre-sub closed within 180 days, one topic, ~10 pages)
and informal-communication criteria (~5,000 characters, one reviewer,
~30 minutes) (highlighted).
### 2. De novo gets performance goals worth planning around
De novo classification has historically been the pathway sponsors avoided because of timeline unpredictability. MDUFA VI changes that calculus:
- MDUFA decision within **150 FDA days for 90% of de novo requests**.
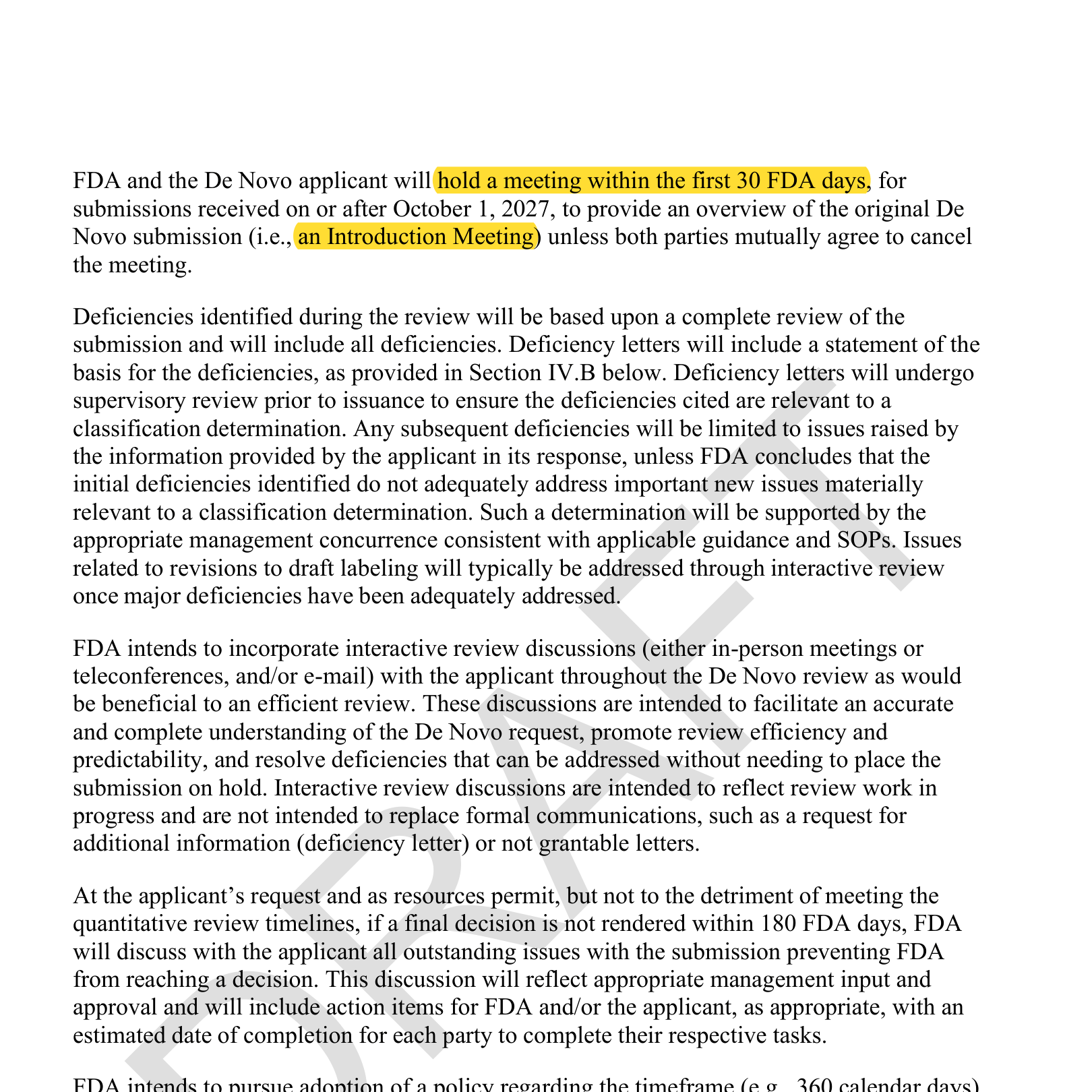
- A new Introduction Meeting within the first 30 FDA days of review, for submissions received on or after October 1, 2027: you present an overview of your submission to the review team at the start, not after the first deficiency letter.
- A de novo--specific pre-submission template, including a clinical study design sub-template, committed for September 2029.
- If you receive a not-grantable letter, FDA intends to render a final determination within 75--90 calendar days of your response.
**What to do:** Revisit de novo as an offensive strategy. The first company through a de novo gets a de facto exclusivity window: competitors must wait for the classification order and decision summary to publish before they can follow via 510(k), and the de novo sponsor negotiates the special controls everyone after them must meet. Timeline risk was the main argument against this play. MDUFA VI substantially reduces it.
One honest caveat: for genuinely novel technology, the bottleneck is usually the clinical study, not FDA\'s review clock. If your device never existed before, expect a prospective, IRB-approved trial. No MDUFA goal shortens that. The 150-day commitment de-risks the part of the timeline you don\'t control; it doesn\'t shrink the part you do.
Source: draft MDUFA VI commitment letter, p. 9 — De Novo decision within
150 FDA Days for 90% of requests; not-grantable final determination
within 75–90 calendar days (highlighted).
Source: draft MDUFA VI commitment letter, p. 10 — De Novo Introduction
Meeting within the first 30 FDA days (highlighted).
### 3. Deficiency quality becomes a permanent floor, and you get leverage
The core deficiency discipline (letters based on a complete review with all deficiencies at once, follow-up deficiencies limited to issues your response raises, ISO 2859-1-audited quality) carries over from MDUFA V. What changes is that the bar stops moving and new accountability arrives:
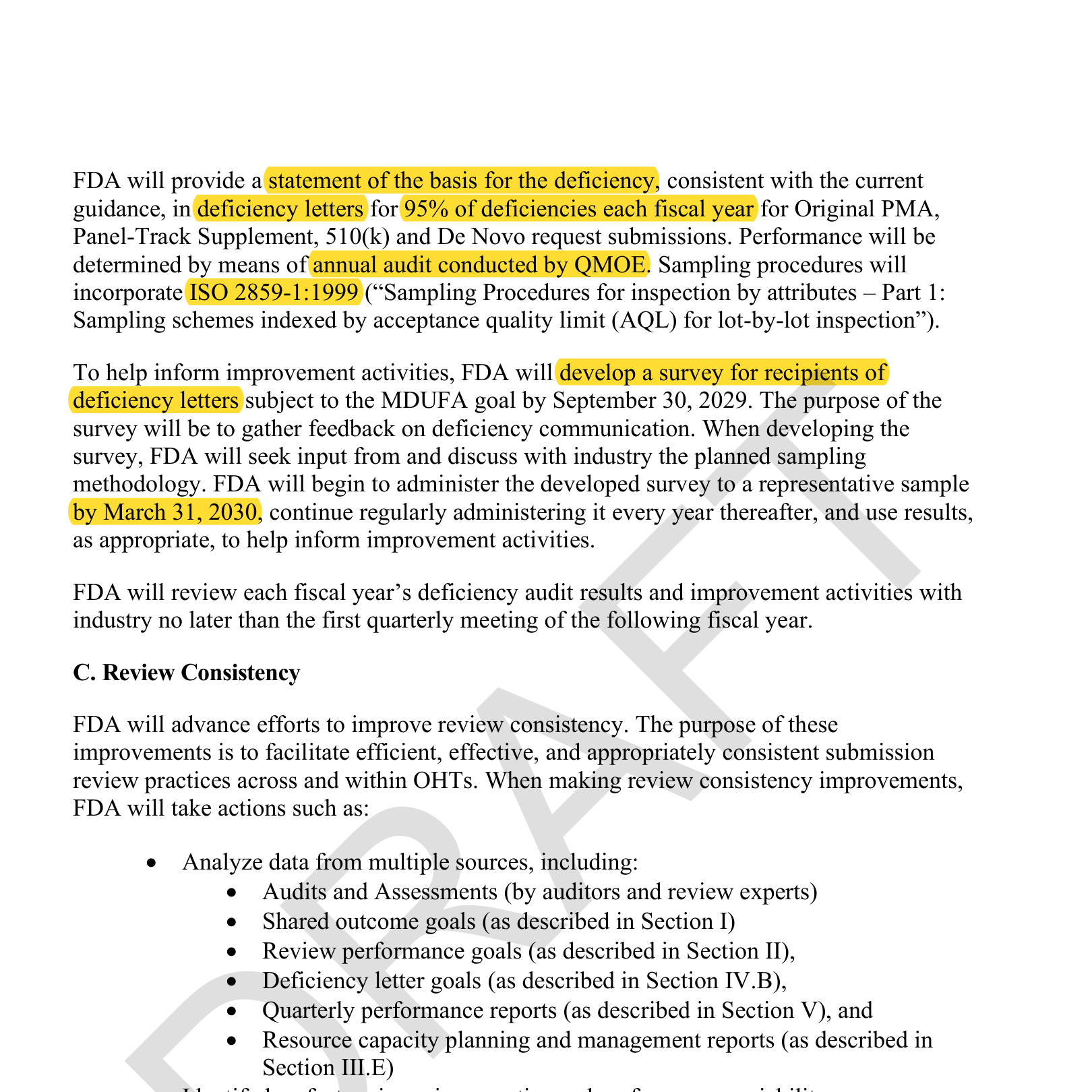
- **95% of deficiencies must state their basis, every year.** MDUFA V phased this in (75% in FY2023, reaching 95% only in FY2027); the draft makes 95% the permanent floor, verified by annual independent audit.
- **New: a survey of deficiency letter recipients**, developed by September 2029, administered from 2030, with results feeding improvement activities.
- **New: a review-consistency program.** FDA must improve at least one high-impact consistency topic per year (at least eight over five years), chosen from a prioritized list industry submits annually.
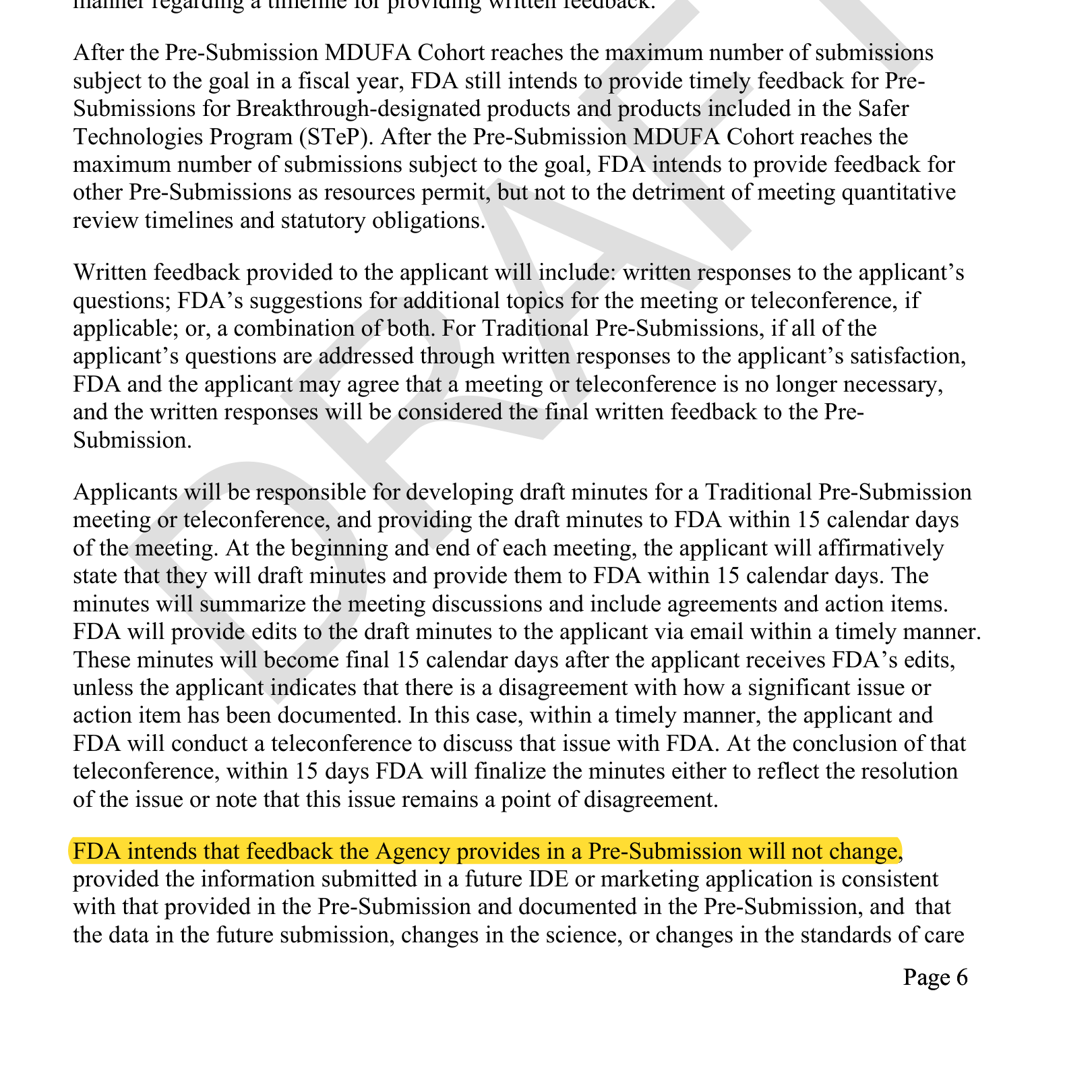
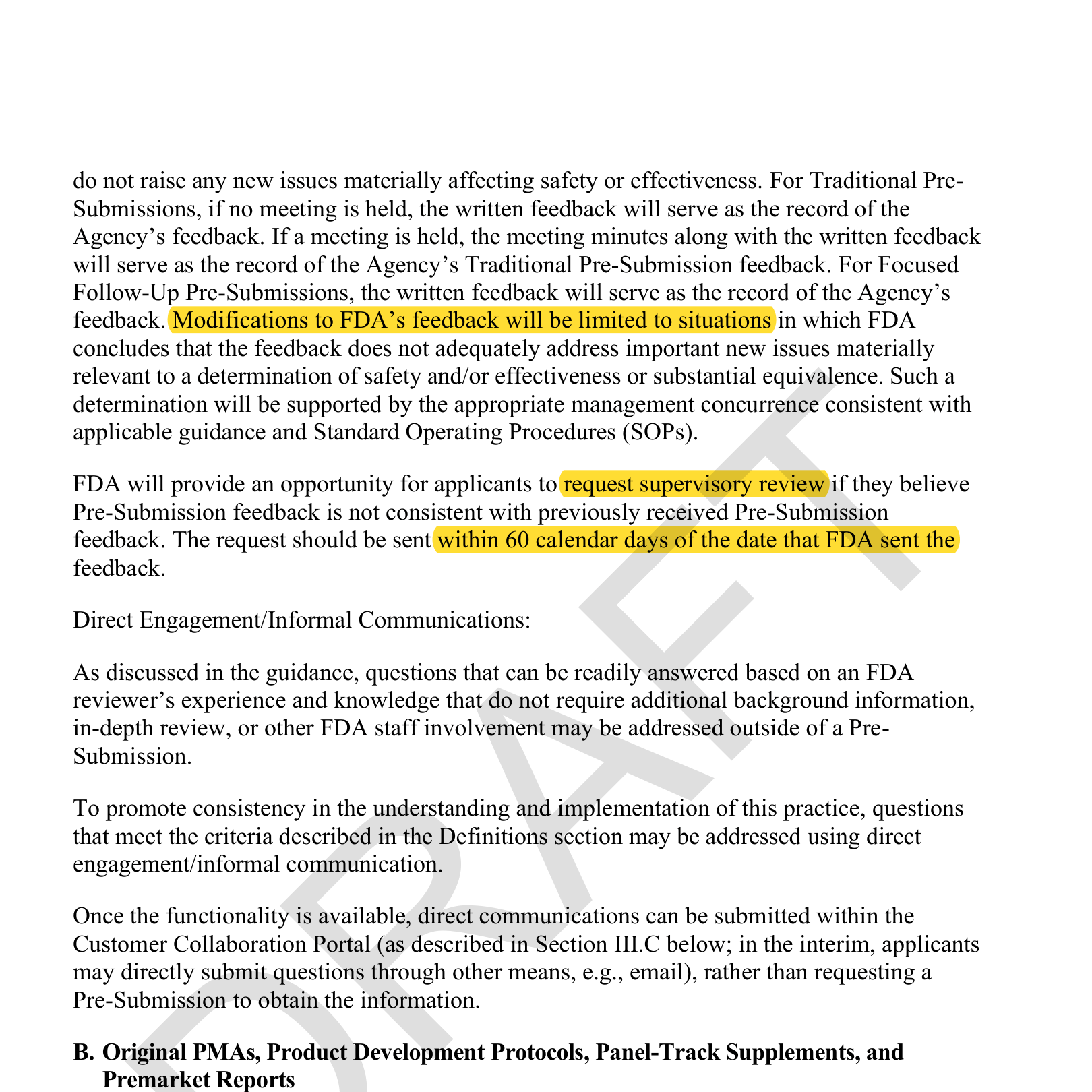
- **New: an explicit escalation right for pre-sub feedback.** The commitment that feedback won\'t change (if your submission stays consistent) also carries over from V, but the draft adds something V lacked: you can formally request supervisory review within 60 days when new feedback contradicts prior feedback.
(The complete-review rule and the limit on mid-review goalpost moves exist in the current deal too: worth knowing, because many sponsors never invoke them.)
**What to do:** Document everything. Under this regime, a well-run pre-sub record becomes an enforceable asset: if a reviewer moves the goalposts, you now have both a paper trail and a formal escalation path. And when a deficiency arrives without a clear stated basis, that\'s no longer just frustrating; it\'s an audit finding.
Two more habits worth building. FDA now uses AI-assisted tools in review, so simulate that adversarial review yourself before you submit, and you won\'t need FDA to tell you where you\'re wrong. And don\'t confuse clearer deficiencies with fewer deficiencies: for novel technology, expect FDA to object to the first study regardless of quality. Plan roughly half the evidence budget for the first round and reserve the rest for the supplemental study that answers the deficiency.
Source: draft MDUFA VI commitment letter, p. 17 — statement of basis for
95% of deficiencies, annual QMOE audit under ISO 2859-1, and recipient
survey administered by March 31, 2030 (highlighted).
Source: draft MDUFA VI commitment letter, p. 6 — FDA intends
Pre-Submission feedback will not change if the future submission is
consistent (highlighted).
Source: draft MDUFA VI commitment letter, p. 7 — feedback modifications
limited; supervisory review may be requested within 60 calendar days
(highlighted).
### 4. Generative and agentic AI are now in the commitment letter
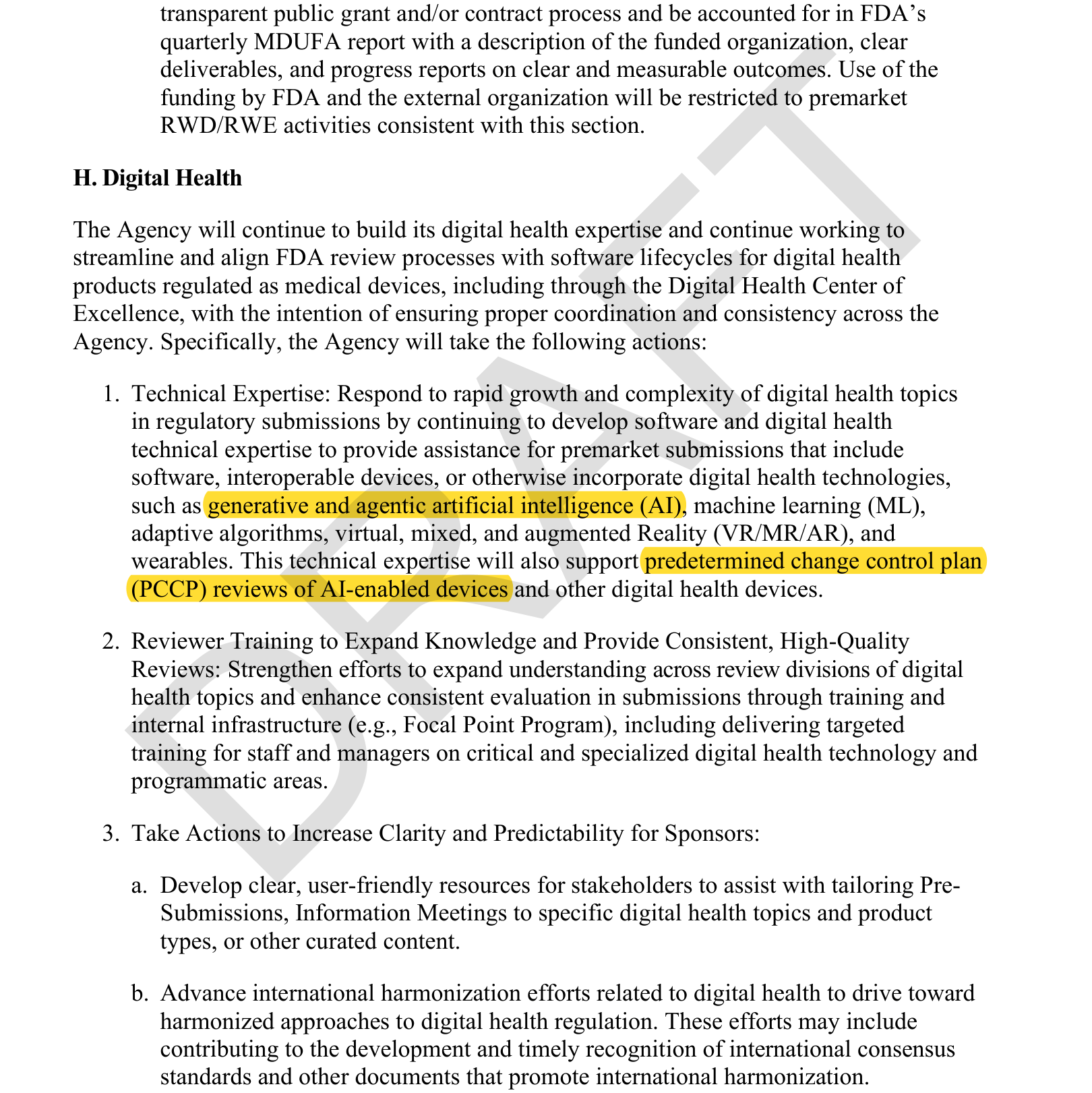
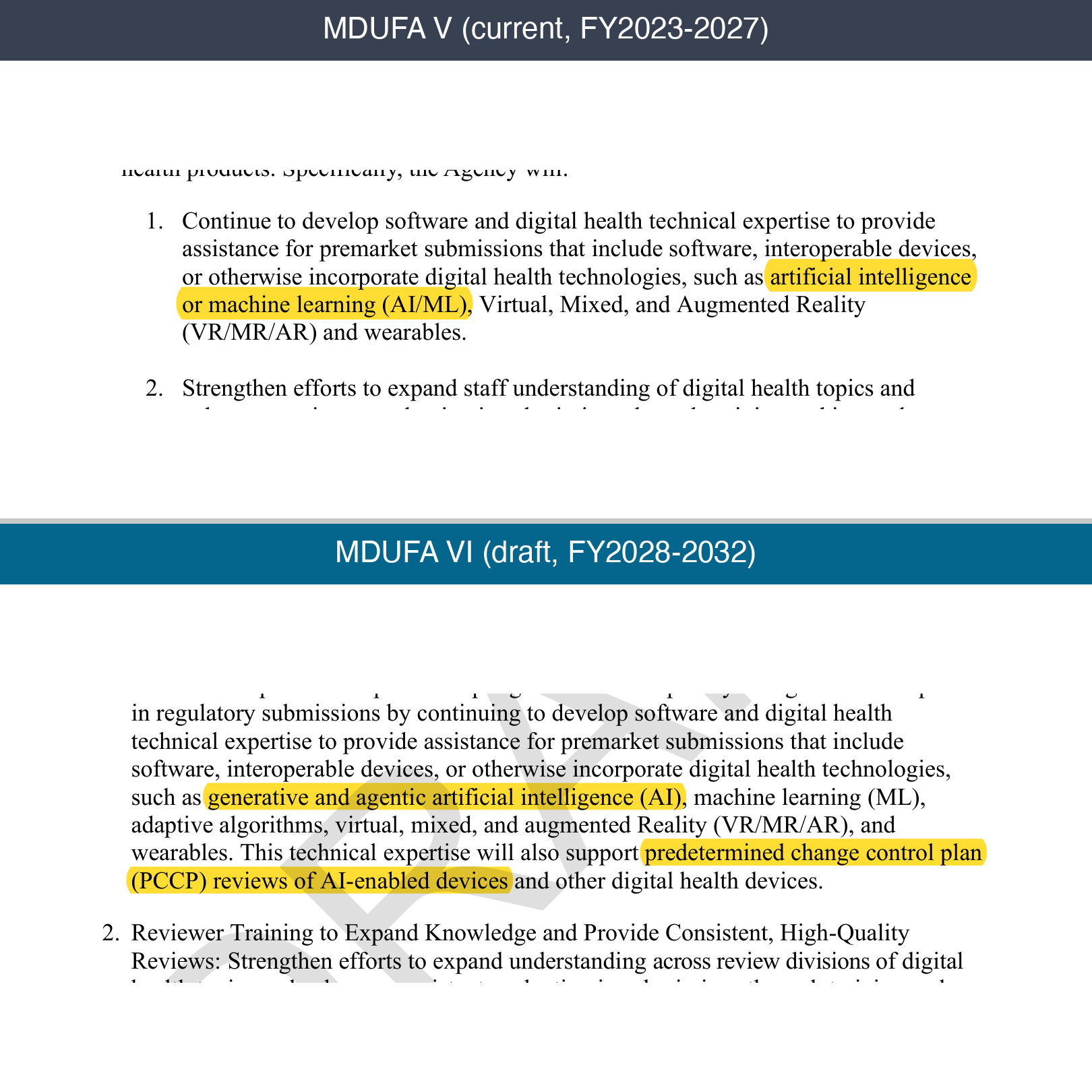
For the first time, a MDUFA letter explicitly names \"generative and agentic artificial intelligence\" as areas where FDA will build technical review expertise, alongside adaptive algorithms, VR/AR, and wearables. FDA also commits to:
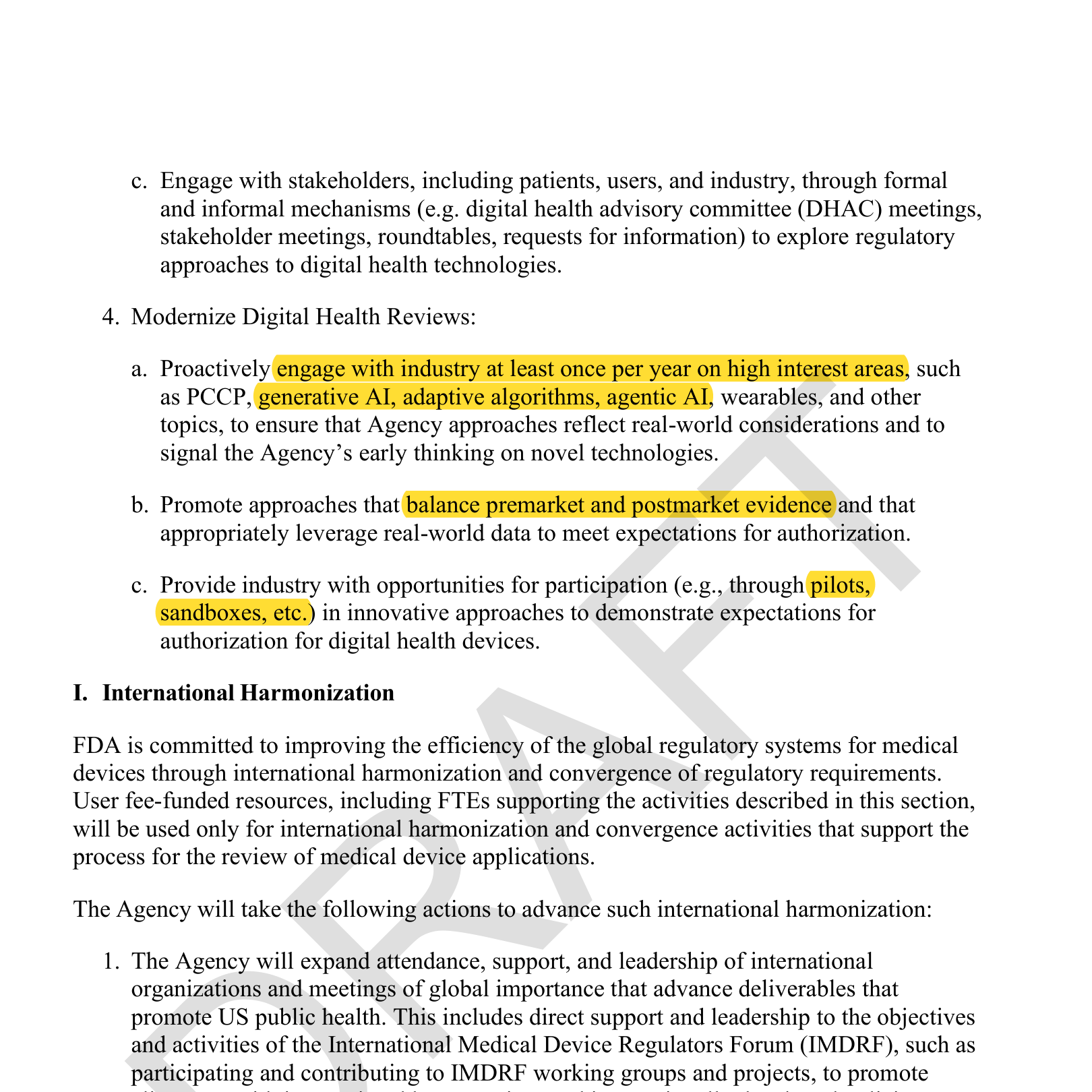
- Engage industry at least once per year on high-interest areas including PCCPs, generative AI, adaptive algorithms, and agentic AI.
- **Offer pilots and sandboxes** for sponsors to demonstrate what authorization requires for novel digital health devices.
- Promote approaches that balance premarket and postmarket evidence, explicitly leveraging real-world data to meet authorization expectations.
**What to do:** If you\'re building an LLM-based or adaptive device, the pathway is maturing but not yet paved. The premarket/postmarket balance language validates the strategy of proposing strong postmarket surveillance as part of the initial submission rather than trying to pre-validate every possible input. They have appeared to have listened to my comments at the first generative AI digital health advisory meeting way back in 2024. Watch for the sandbox programs (and/or sign up for our newsletter so we can alert for you); early participants will shape the expectations everyone else inherits.
The premarket/postmarket balance language gives official cover to a negotiating position that already works: offer postmarket prospective activities as a bargaining chip against up-front evidence demands. Premarket, prove the device isn\'t unsafe; push efficacy measurement into the postmarket, where real-world use can show what a fabricated study environment can\'t. You can\'t pre-validate every input to a generative system, and this language is FDA conceding the point.
Source: draft MDUFA VI commitment letter, p. 23 — "generative and
agentic artificial intelligence (AI)" named as review expertise areas,
including PCCP reviews of AI-enabled devices (highlighted).
Source: draft MDUFA VI commitment letter, p. 24 — annual industry
engagement on generative AI, adaptive algorithms, agentic AI; pilots and
sandboxes; balancing premarket and postmarket evidence (highlighted).
### 5. Real-world evidence: the sleeper section of the whole letter
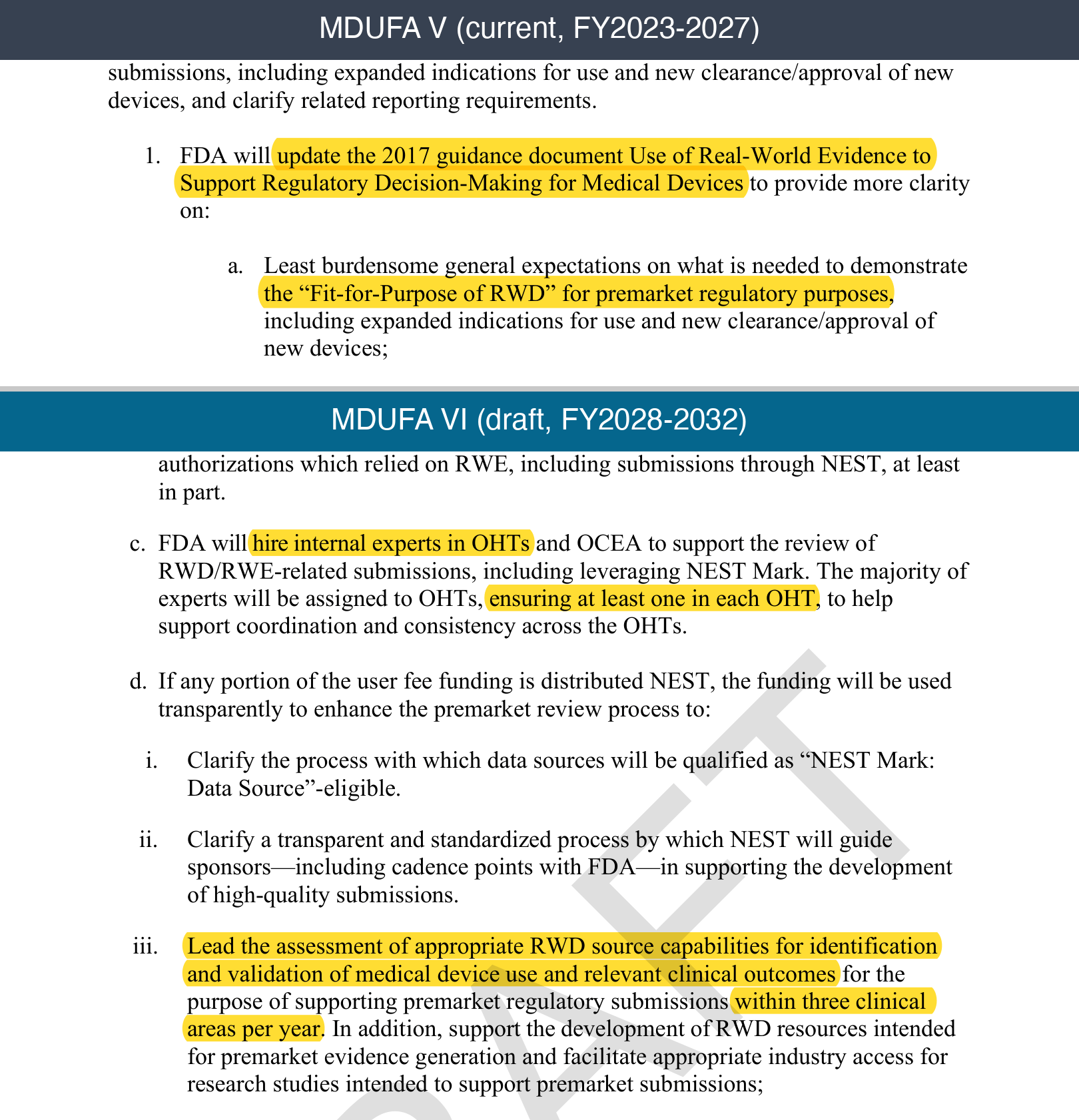
The reason RWE hasn\'t delivered on that promise: reviewers couldn\'t trust the data sources, and couldn\'t map retrospective designs onto familiar frameworks. MDUFA V tried to fix this with policy: its RWE section promised an update to the 2017 RWE guidance (\"Fit-for-Purpose of RWD\"), training, and public meetings. Guidance clarifies; it doesn\'t unblock. The MDUFA VI draft builds infrastructure instead:
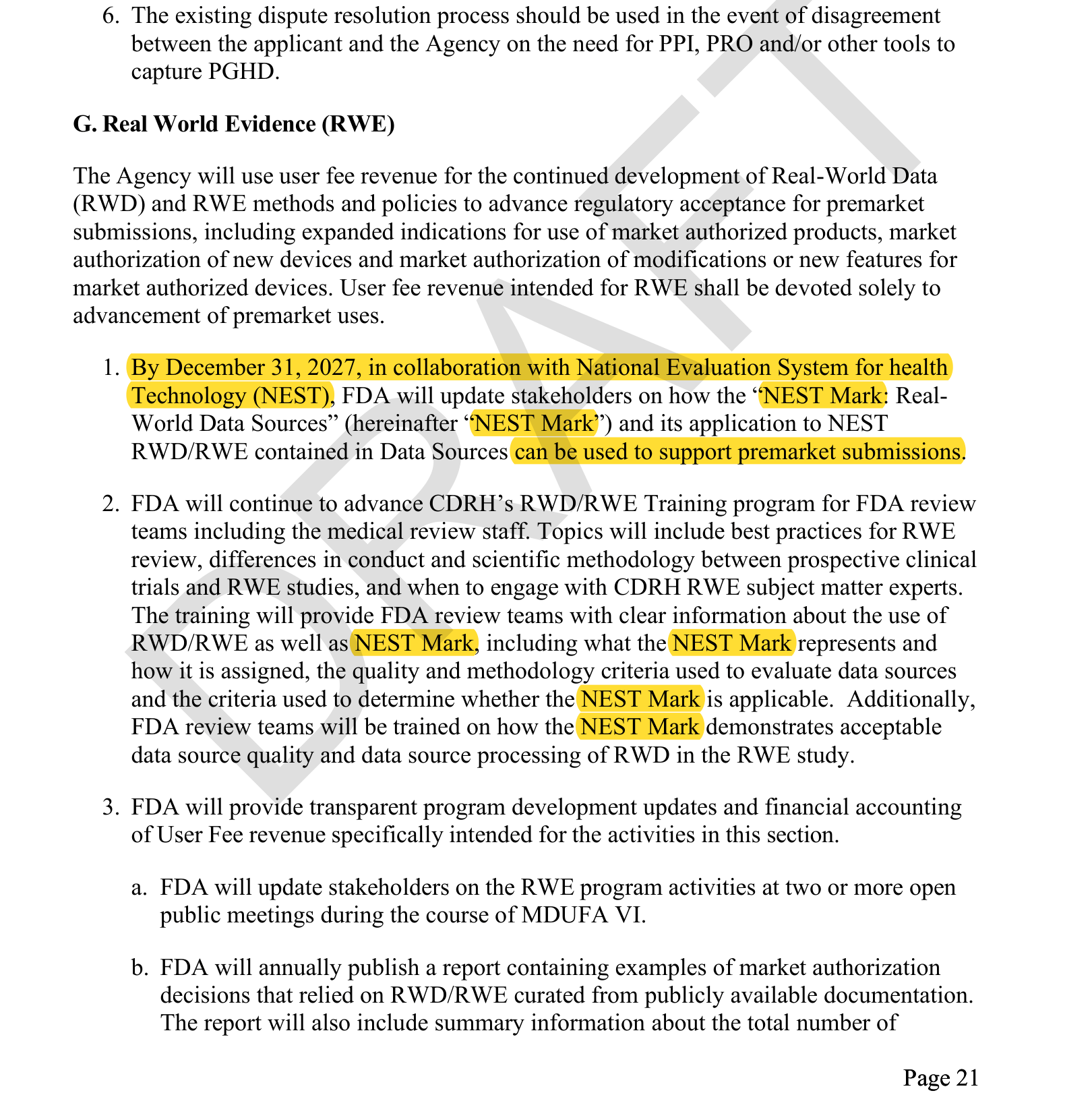
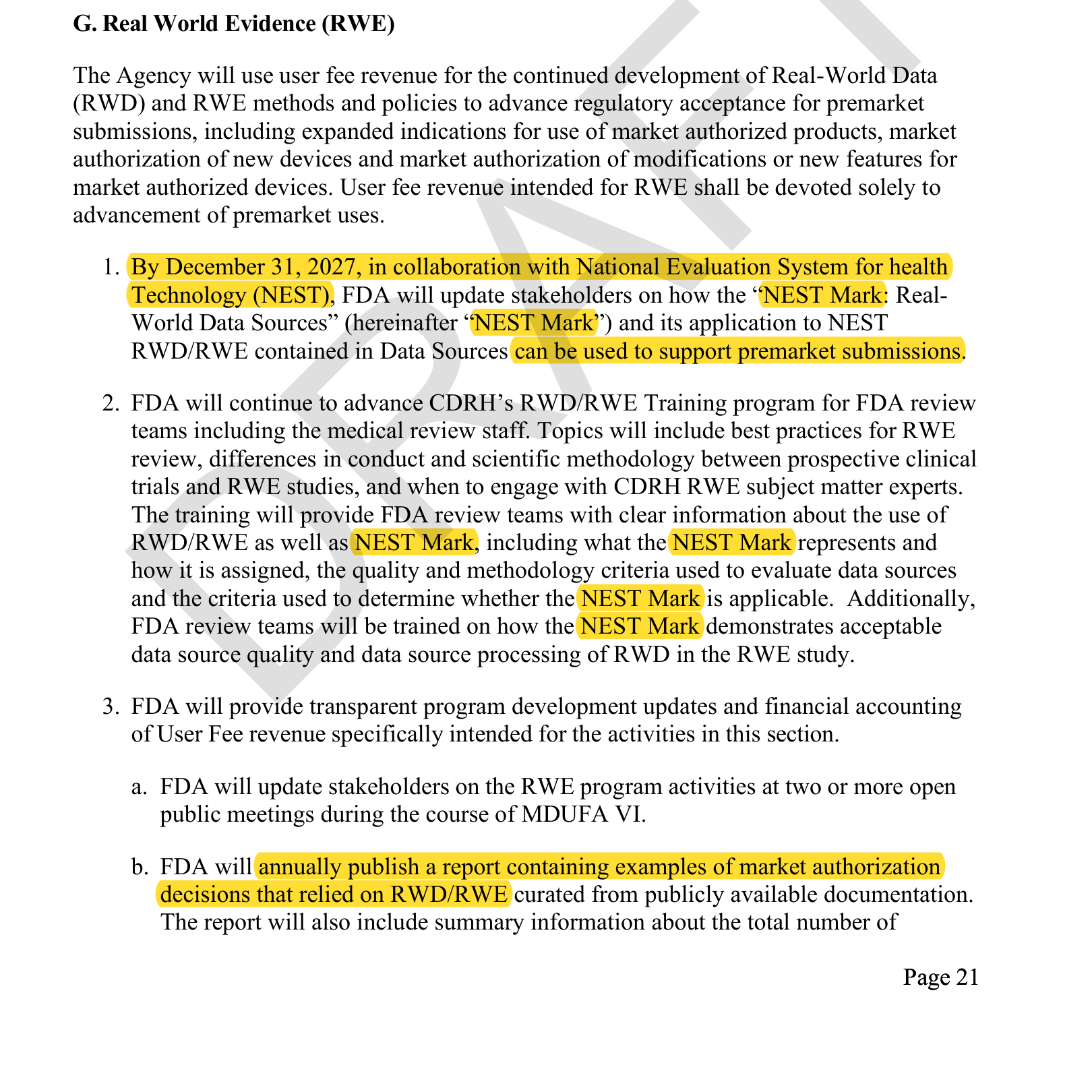
- **The NEST Mark**: a qualification designation for real-world data sources, with a stakeholder update committed by December 31, 2027. A pre-validated answer to the reviewer\'s first objection: \"why should I trust this data?\"
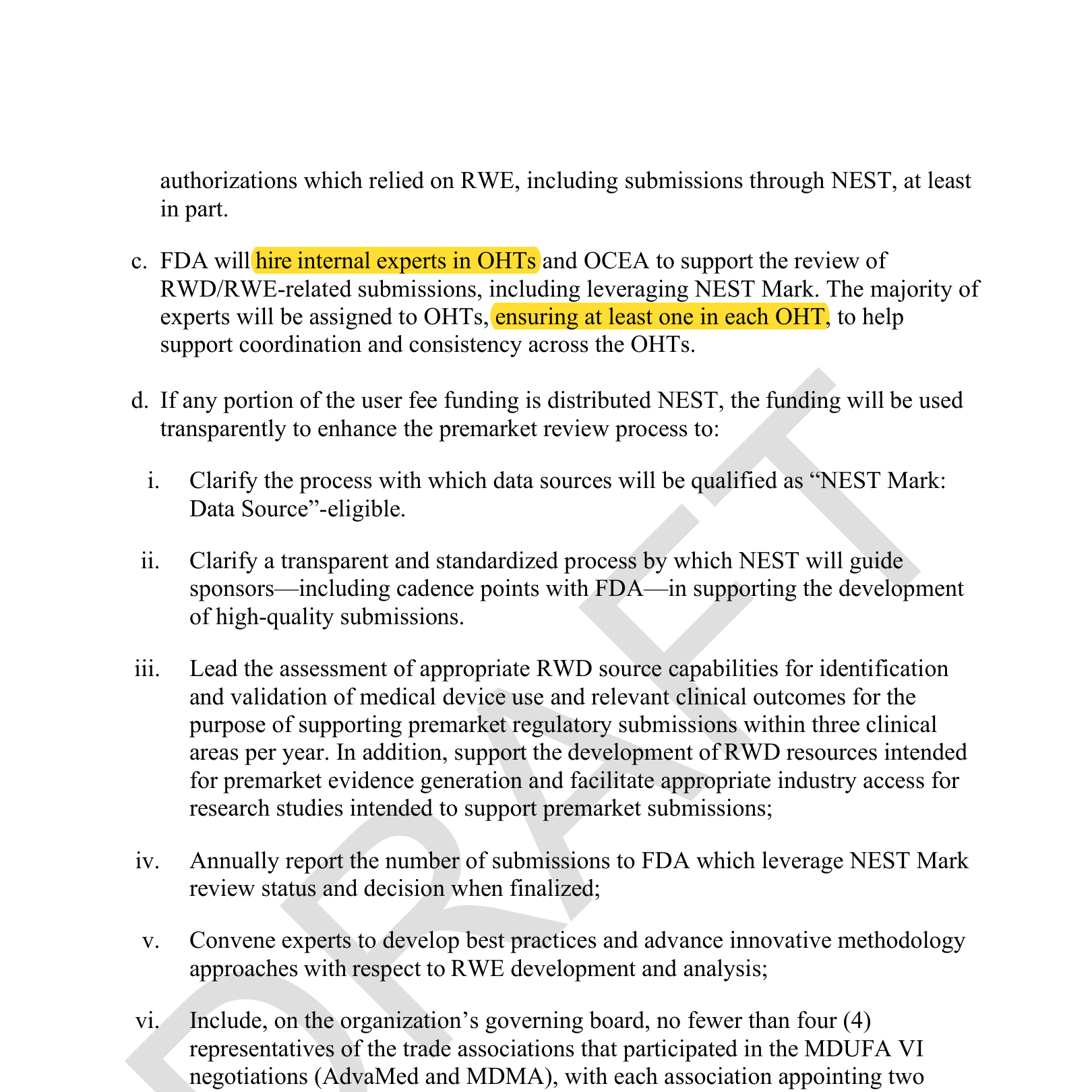
- **Outcome-as-label machinery.** NEST will lead \"the assessment of appropriate RWD source capabilities for identification and validation of medical device use and relevant clinical outcomes\" for premarket submissions, three clinical areas per year. That is the agency-side plumbing for the ground-truth-free design: validated outcomes in the data replacing paid readers.
- **An RWE expert in every OHT, and reviewers trained on the methodology gap.** The most common failure mode for retrospective submissions (a review team that has never seen one) gets a structural fix: a subject-matter expert inside each review office, plus mandatory reviewer training on \"differences in conduct and scientific methodology between prospective clinical trials and RWE studies\" and on when to pull in the RWE experts. FDA is teaching its reviewers the exact framework distinction that retrospective submissions die on today.
- **A standardized sponsor process.** NEST will run a transparent process guiding sponsors, including cadence points with FDA, toward high-quality RWE submissions.
- **An annual precedent library.** FDA will publish a yearly report of marketing authorizations that relied on RWE. Precedent is how you argue a less-burdensome path; this report writes the citations for you.
- **Premarket-only funding.** User-fee RWE money is restricted \"solely to advancement of premarket uses\": aimed at getting devices authorized, not just surveilled.
**What to do:** If you\'re validating an AI device, price the RWE path before you price the reader study. Run a retrospective pilot on real-world data first to learn where performance stands before committing to an expensive adjudicated study. Track which data sources earn the NEST Mark, design endpoints around outcomes the data already captures, and frame the study within FDA\'s RWE guidance so reviewers recognize the shape of it.
Two disciplines the new infrastructure doesn\'t change. Claims language: retrospective evidence supports a claim, it never proves one: you cannot use \"prove\" and \"emulate\" in the same sentence, and a qualified data source doesn\'t alter that. And confounding: state explicitly in the pre-sub that you will correct for selection bias between groups. You don\'t need the full adjustment plan yet, but you need the commitment on record.
MDUFA V printed p. 20 (promise to update the 2017 RWE guidance,
"Fit-for-Purpose of RWD") vs. draft MDUFA VI p. 22 (NEST validates
device use and clinical outcomes in RWD sources, three clinical areas
per year; RWE expert in every OHT).
Source: draft MDUFA VI commitment letter, p. 21 — NEST Mark update to
stakeholders by December 31, 2027 for supporting premarket submissions
(highlighted).
Source: draft MDUFA VI commitment letter, p. 21 — annual public report
of authorizations that relied on RWD/RWE (highlighted).
Source: draft MDUFA VI commitment letter, p. 22 — internal RWD/RWE
experts hired, at least one in each OHT (highlighted).
### 6. The review clock is shared, and FDA publishes your side of it
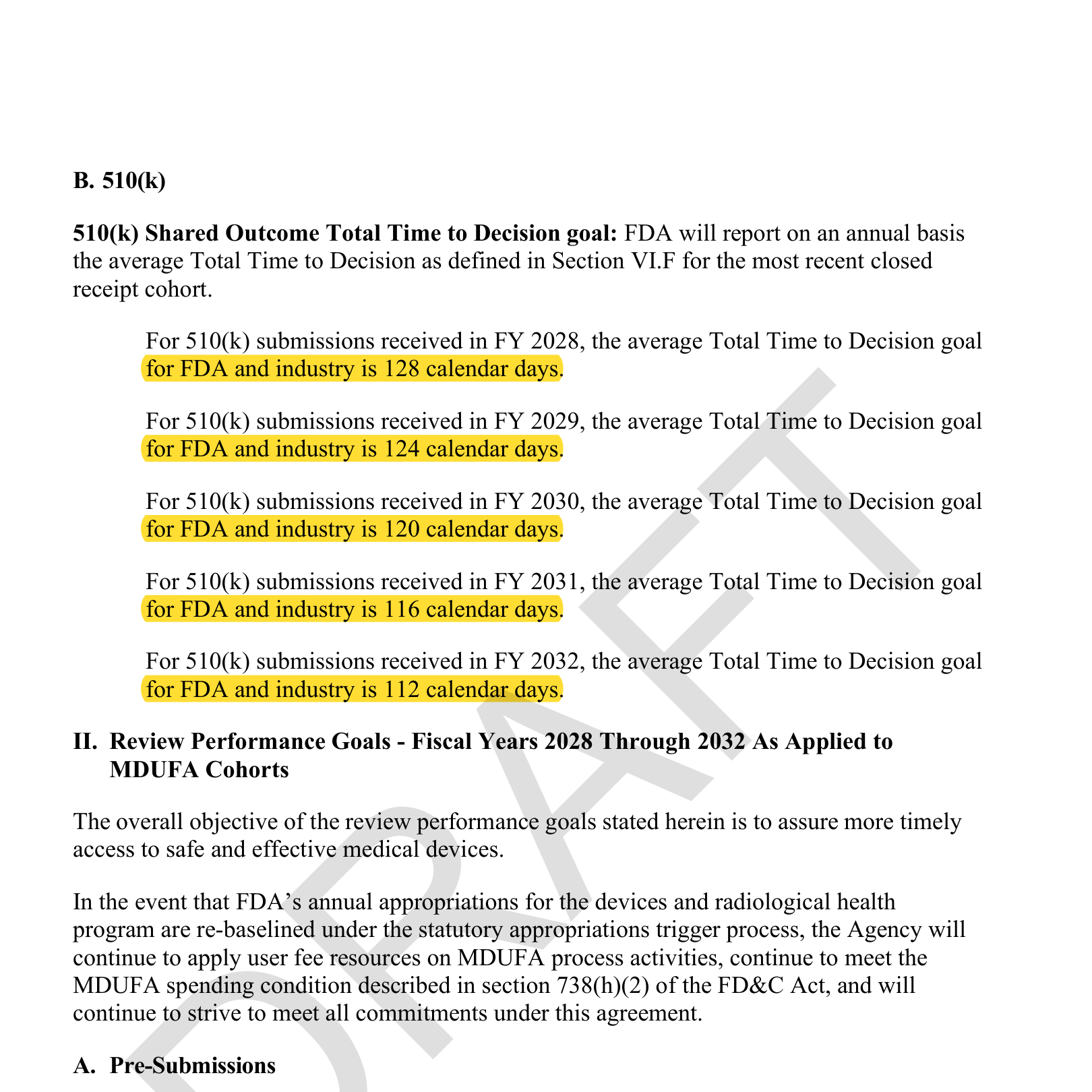
The headline goals: average total time to decision for 510(k)s starts at 128 days in FY2028 and steps down to 112 days by FY2032; PMA panel-track average is 285 days. So yes, the goal drops over the life of the deal. But don\'t read that ladder as FDA promising faster reviews, because the baseline moved. The current deal already promised 112 days by FY2025. The new one restarts at 128 and takes until FY2032 to get back to a number FDA was supposed to hit three years ago.
What that means in business terms. If you own the P&L: build launch dates and runway on roughly four months of 510(k) review calendar (plus your own response time), and treat anything faster as upside, not plan. If you invest in this space: committed review speed is flat through 2032, the stretch goals that could have improved it were deleted from the deal, so time-to-revenue assumptions for device startups should not shorten on the basis of this agreement.
The other thing to know about these numbers: they are shared outcome goals, and your side of the clock is public. A review alternates between FDA days (the file is with the agency) and industry days (the file is on hold while you prepare a response to a deficiency letter). The goals count both halves, and FDA reports them separately in its public performance data, so a sponsor that sits on a hold letter for 90 days shows up in the numbers as exactly that (a structure carried over from MDUFA V, which has been quietly making sponsor response time visible for years).
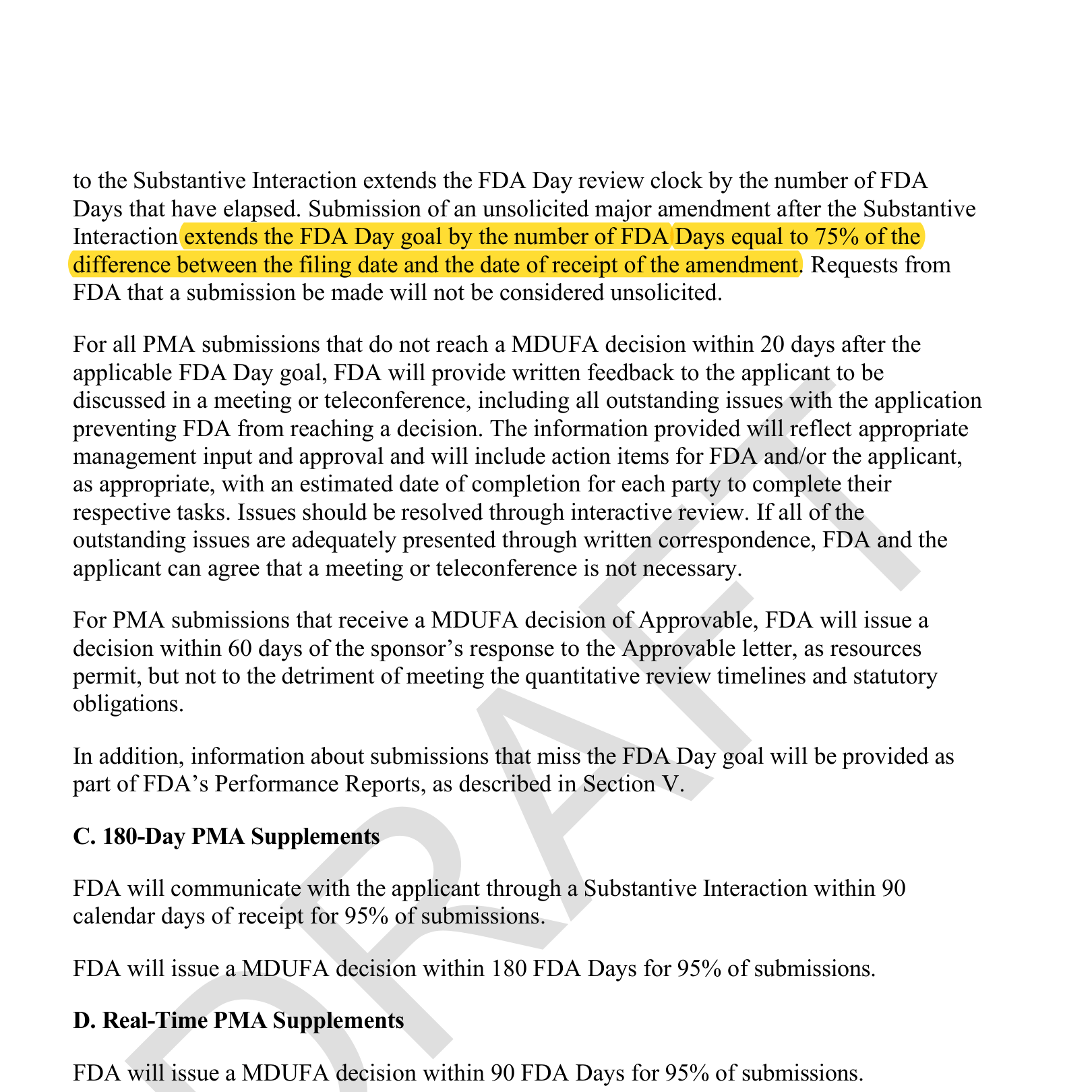
Two mechanics to plan around (both carried over from the current deal, both still underappreciated):
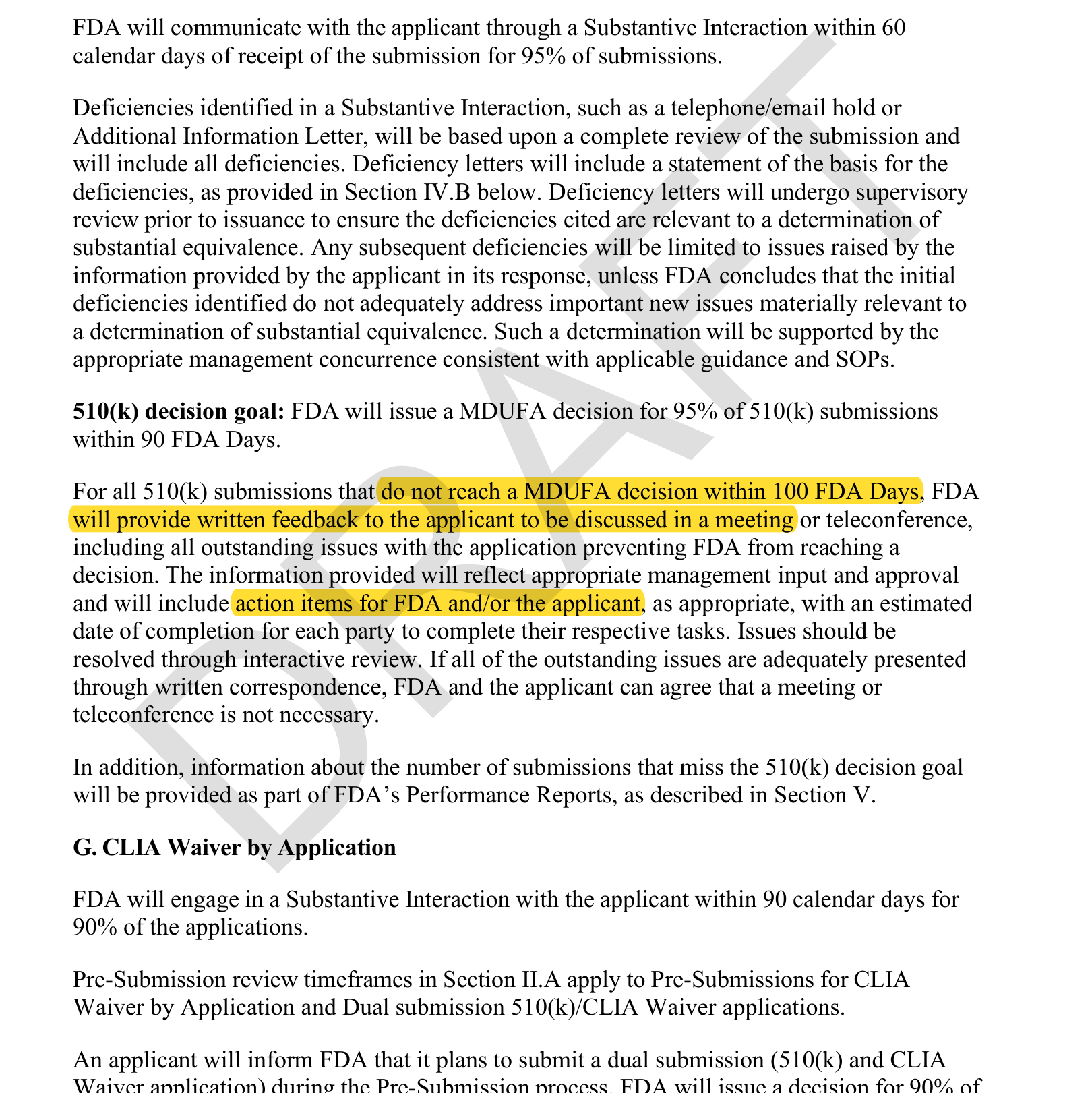
- For PMAs, an unsolicited major amendment after the Substantive Interaction extends the review clock by 75% of the days already elapsed: an explicit, quantified penalty for incomplete filings.
- Any 510(k) still undecided at 100 FDA days gets mandatory written feedback and a meeting with action items and due dates for both parties.
**What to do:** Submission completeness is a measured metric, and under a shared-outcome regime your response time is part of the published number. Never submit with visible failing endpoints or known gaps you plan to patch mid-review. Set defensible acceptance criteria before you submit, not after FDA flags a failure.
But completeness is not perfectionism. The right move is usually to submit on time with the data you have and a defensible justification (keeping the backup study as a documented plan B) rather than delay months waiting for certainty FDA may never demand. Calculated risks like this routinely shave weeks off submissions; the discipline is knowing which gaps are defensible and which will read as a visible fail.
Source: draft MDUFA VI commitment letter, p. 4 — 510(k) shared outcome
Total Time to Decision ladder: 128 days (FY2028) stepping down to 112
days (FY2032) (highlighted).
Source: draft MDUFA VI commitment letter, p. 9 — unsolicited major
amendment extends the FDA Day goal by 75% of elapsed days (highlighted).
Source: draft MDUFA VI commitment letter, p. 11 — 510(k)s not decided
within 100 FDA Days get written feedback and a meeting with action items
(highlighted).
### 7. Breakthrough devices: TAP goes program-wide, with CMS at the table
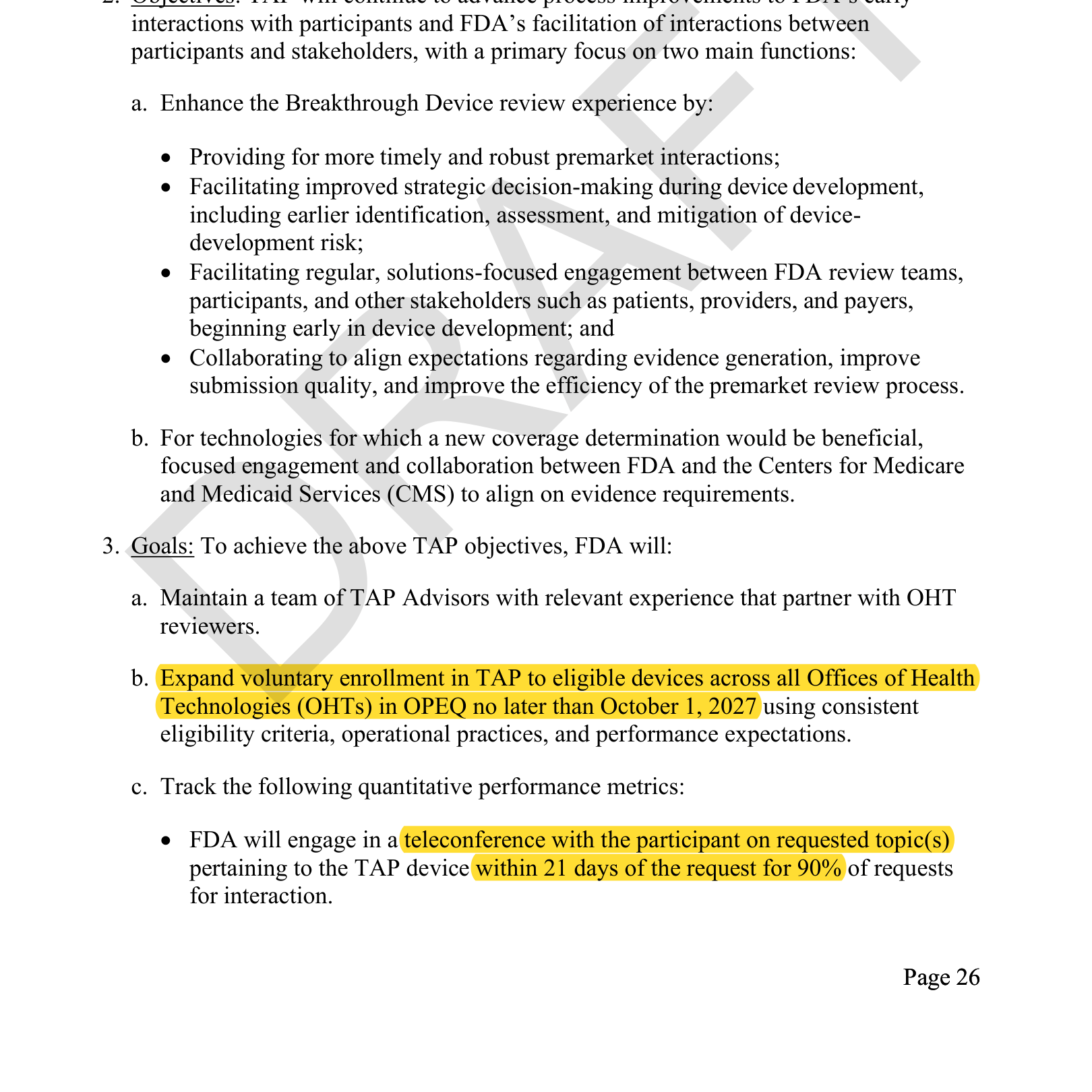
The Total Product Life Cycle Advisory Program (TAP) exits pilot status and expands to all OHTs by October 1, 2027 for Breakthrough-designated devices, with quantitative goals:
- Teleconference on requested topics within **21 days** for 90% of requests.
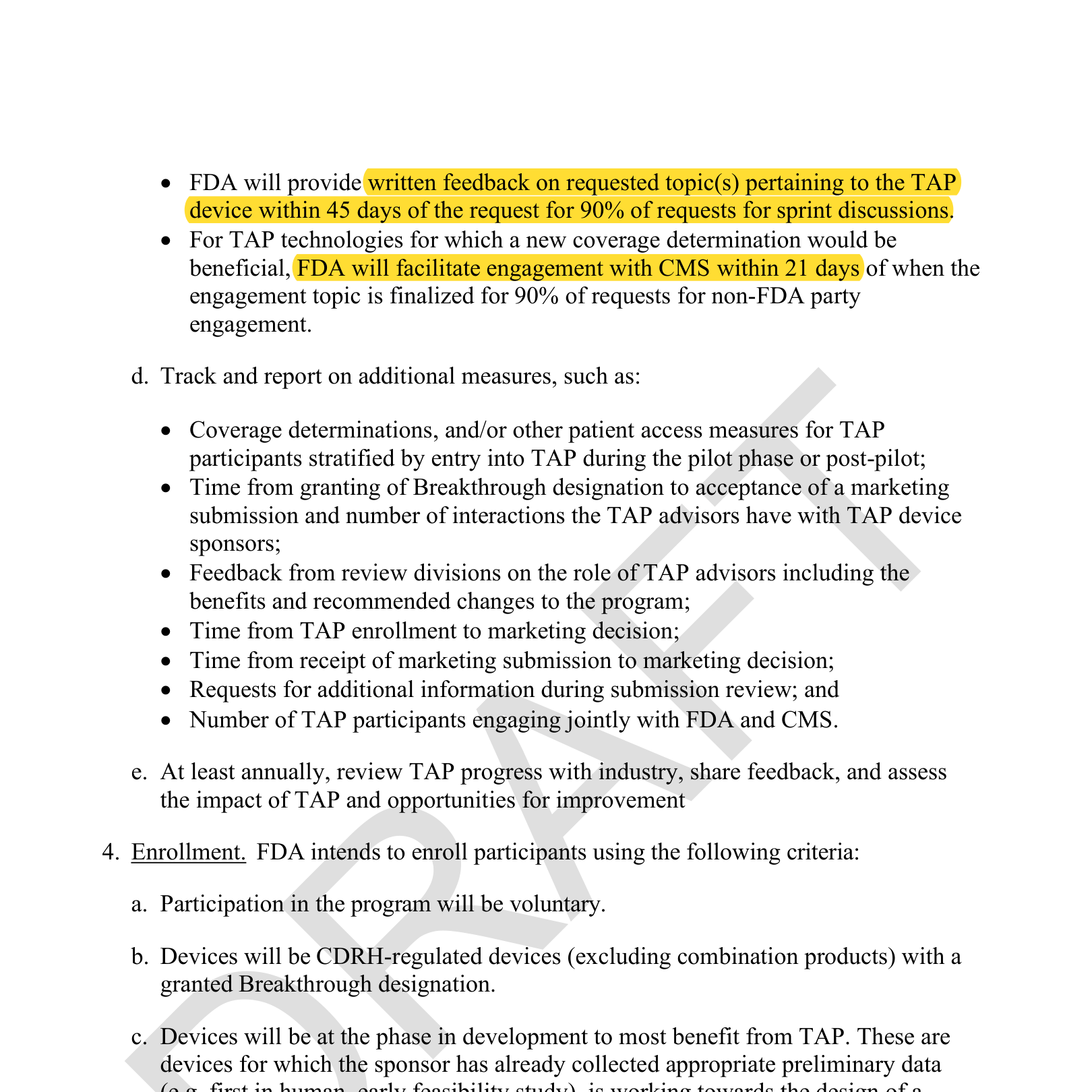
- Written sprint feedback within **45 days** for 90% of requests.
- For technologies where a new coverage determination would help, FDA will facilitate **CMS engagement within 21 days** of finalizing the topic.
**What to do:** Breakthrough designation\'s known benefits were review priority and market optics. TAP adds the commercially decisive one: structured reimbursement alignment while you\'re still designing the pivotal study. If your device plausibly qualifies for Breakthrough and a pivotal study is on your roadmap within \~24 months, TAP enrollment should be part of the regulatory plan, and your evidence strategy should be designed for two audiences, FDA and CMS, from day one.
Note what the enrollment criteria are really telling you: FDA has grown more conservative on Breakthrough, expecting believable preliminary data that the claimed performance is plausibly achievable before granting anything. TAP\'s preliminary-data-in-hand, pivotal-within-24-months window writes that conservatism into policy. Don\'t file the designation request before your algorithm is at a testable stage: a denial is worse than a delay.
Source: draft MDUFA VI commitment letter, p. 26 — TAP enrollment
expanded to all OHTs no later than October 1, 2027; 21-day
teleconference goal (highlighted).
Source: draft MDUFA VI commitment letter, p. 27 — 45-day written sprint
feedback and FDA-facilitated CMS engagement within 21 days
(highlighted).
### What changed from MDUFA V, and what it means for your timeline
I also compared the draft line by line against the current MDUFA V commitment letter (FY2023--2027). Skipping the administrative trivia, here are the differences that actually move time to market and business planning. Each claim is shown side by side: the current letter\'s language on top, the draft\'s below, with the supporting text highlighted.
#### The 510(k) clock resets: 2028 looks like 2023
MDUFA V promised a 510(k) average total time to decision of 112 days by FY2025. The draft MDUFA VI ladder restarts at 128 days in FY2028 (the same number V started with in FY2023) and doesn\'t reach 112 again until FY2032. The new deal\'s five-year finish line is where the current deal was supposed to be three years ago, and V\'s 108-day stretch goal is gone entirely.
**What it means:** if your launch model uses \"MDUFA goal\" timelines, stop. Use published actuals. The agencies\' own negotiators just told you the current goals weren\'t holding.
MDUFA V printed p. 2 (112 days due FY2025–2027) vs. draft MDUFA VI p. 4
(restart at 128 days FY2028, 112 not until FY2032).
#### De novo goes from coin-flip to commitment
MDUFA V: decision within 150 FDA days for 70% of de novo requests, a goal you couldn\'t responsibly put in a board deck. MDUFA VI: 90% at the same 150 days, plus the 30-day Introduction Meeting and 75--90-day not-grantable resolution.
**What it means:** de novo timeline risk, the main reason sponsors avoided the pathway and its exclusivity upside, drops enough to change pathway selection math.
MDUFA V printed p. 7 (150 FDA Days for 70%) vs. draft MDUFA VI p. 9 (150
FDA Days for 90%, not-grantable resolved in 75–90 days).
#### Regulatory Q&A cycle time drops by a third
MDUFA V has one pre-sub lane: 70-day written feedback, and the informal-communication option existed only as a promised guidance update. MDUFA VI ships two new lanes with defined mechanics: the 45-day Focused Follow-Up Pre-Sub and the tracked informal channel.
**What it means:** a strategy question that took a 70-day round trip (or got batched into next year\'s pre-sub) becomes a 45-day or same-week answer. Across a development program with three or four FDA touchpoints, that\'s months off the schedule.
MDUFA V printed p. 5 (informal communication promised only as a guidance
update) vs. draft MDUFA VI p. 4 (Focused Follow-Up Pre-Submissions,
written response in 45 calendar days).
#### Review predictability gets a floor, not a ramp
MDUFA V phased in deficiency quality: a statement of basis for 75% of deficiencies in FY2023, reaching 95% only in FY2027. MDUFA VI makes 95% the floor every year, audited, with a recipient survey and a new review-consistency program (at least eight high-impact topics over five years, chosen by FDA from an industry-prioritized list).
**What it means:** surprise deficiencies are the single biggest driver of blown regulatory budgets. A permanent 95% basis requirement plus a consistency program is FDA committing to fewer of them, and giving you standing to push back when one arrives unexplained.
MDUFA V printed p. 17 (basis statement phased 75%→95% by FY2027) vs.
draft MDUFA VI p. 17 (95% every fiscal year, ISO 2859-1 audited).
#### Breakthrough economics change shape
The TAP pilot becomes a permanent program across all OHTs, with FDA-facilitated CMS engagement within 21 days, which didn\'t exist in V at all. Two trade-offs: per-request response goals loosen slightly (teleconference 14→21 days; written feedback 40→45 days), and the enrollment window changes: V wanted devices early (pre-pivotal); VI wants preliminary data in hand and a pivotal study within \~24 months.
**What it means:** the reimbursement bridge means coverage strategy starts during pivotal design, not after clearance. And enrollment timing is now a decision to plan, not a default to grab at designation.
MDUFA V printed p. 25 (pilot metrics: 14-day teleconference, 40-day
written feedback) vs. draft MDUFA VI p. 27 (45-day sprint feedback plus
CMS engagement within 21 days).
#### The stretch goals and the accountability are gone
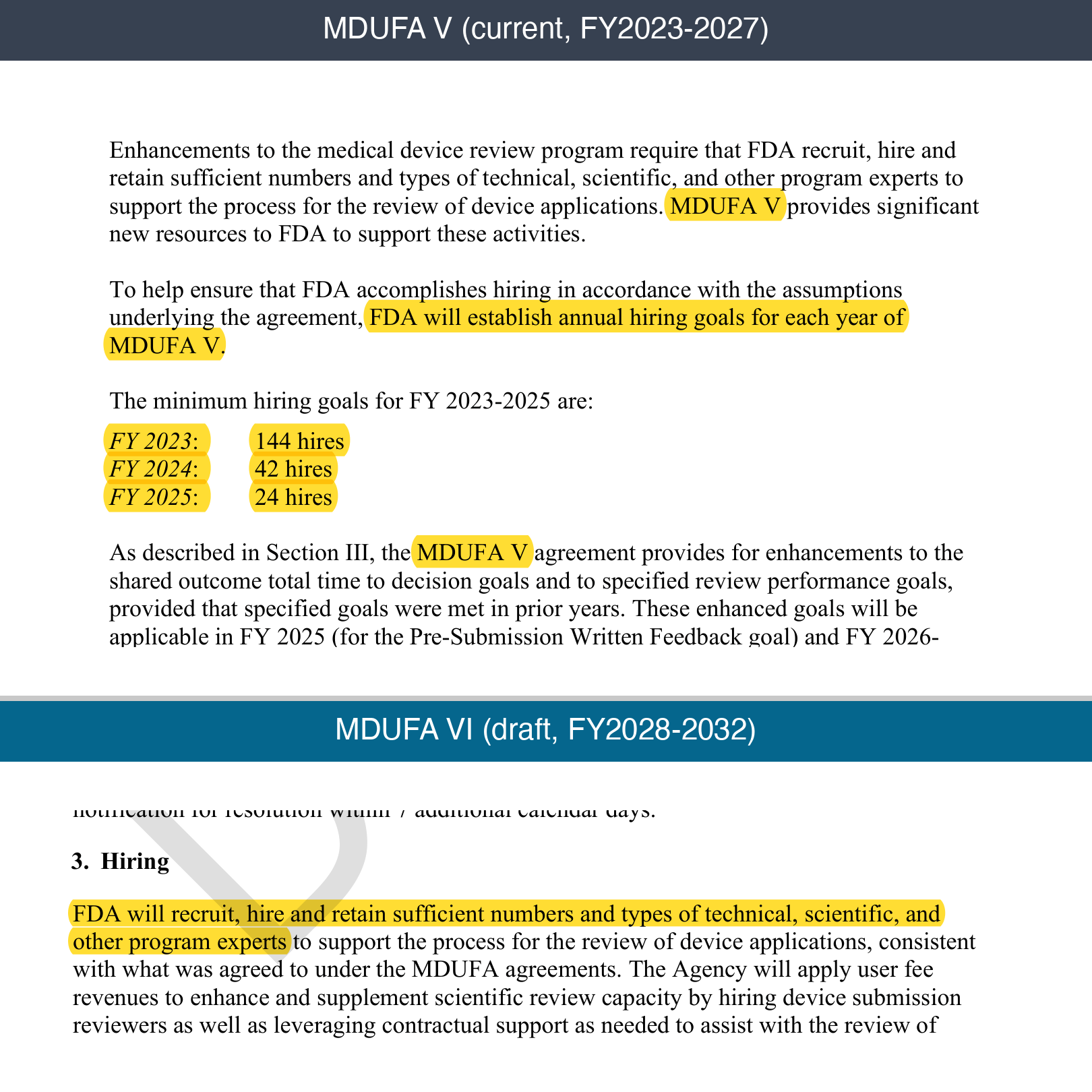
MDUFA V contained trigger machinery: if FDA hit its goals and industry paid more, the 510(k) goal would tighten to 108 days, PMA to 270--275, de novo to 90%. It also set numeric hiring goals (144/42/24 hires) with a fee-refund penalty for missing them. MDUFA VI deletes all of it: flat goals, no enhancements, no hiring numbers, no fee penalty.
**What it means:** the printed goals are the ceiling, not the floor. Build plans on the numbers as written; there is no upside scenario coming.
MDUFA V printed pp. 14–15 (annual hiring goals: 144/42/24 hires, fee
adjustment if missed) vs. draft MDUFA VI p. 14 ("sufficient numbers" —
no numeric goals, no penalty).
#### One evidence package, multiple regulators
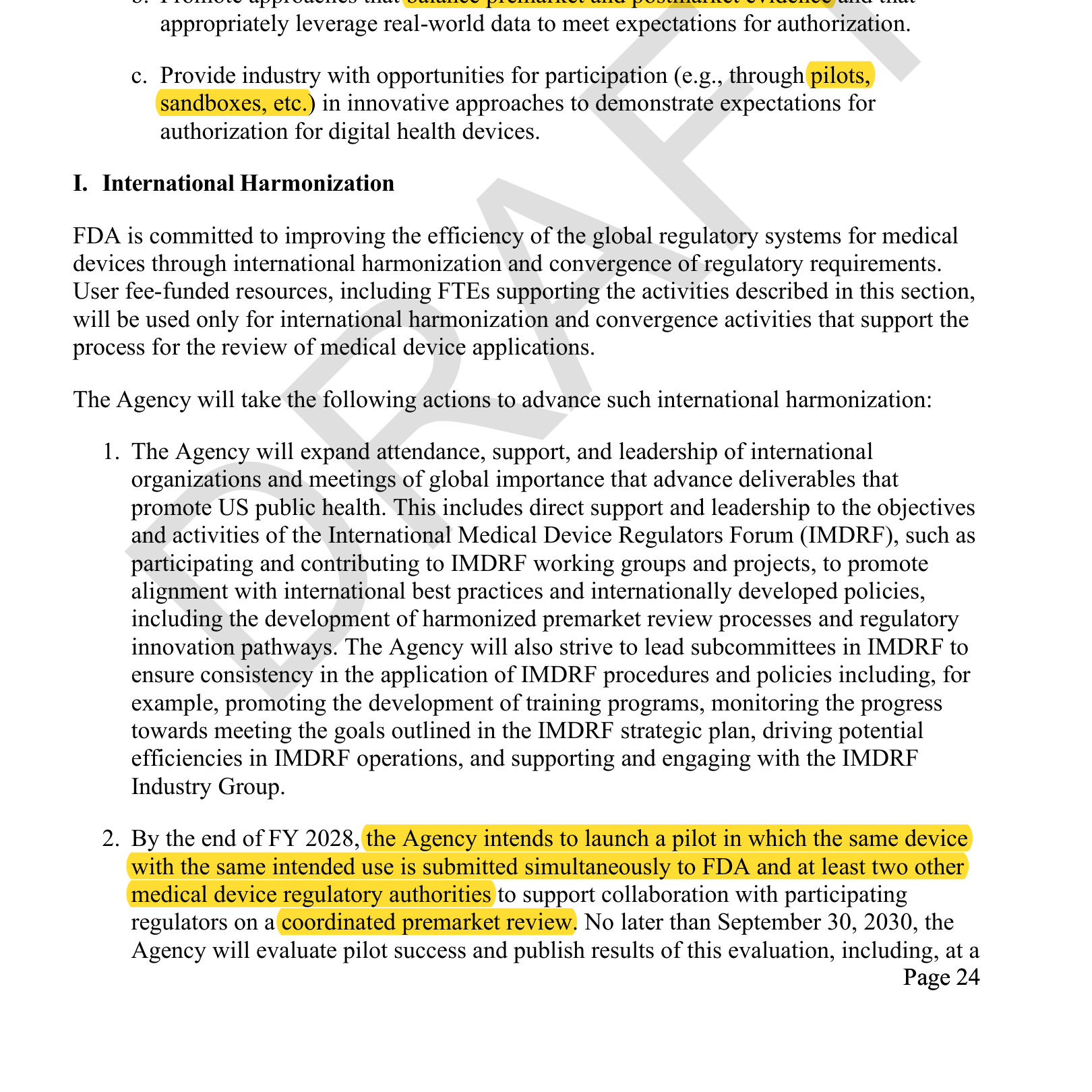
Buried in the international section: by the end of FY2028, FDA intends to launch a pilot in which the same device with the same intended use is submitted simultaneously to FDA and at least two other regulatory authorities for a coordinated premarket review, with results published by 2030, including feasibility of a future single-review program. Alongside it, FDA commits to an abridged-reliance approach: leveraging elements of a trusted foreign regulator\'s scientific assessment (where confidentiality commitments exist) while keeping the final decision. MDUFA V\'s international section was participation and strategic plans; this is operational machinery.
**What it means:** the same economics that make real-world evidence attractive apply here: build the evidence package once, use it N times. If you\'re planning FDA plus EU (or Japan, or Canada) within the same program, watch this pilot: early participants get one coordinated review instead of sequential, divergent question sets, and the published results will show exactly where the regulators\' expectations align and diverge.
Draft MDUFA VI p. 24 — pilot: same device, same intended use, submitted
simultaneously to FDA and at least two other regulatory authorities for
coordinated premarket review (highlighted).
#### AI: from model artifact to living system
MDUFA V\'s digital health language: \"artificial intelligence or machine learning (AI/ML).\" MDUFA VI: \"generative and agentic artificial intelligence,\" adaptive algorithms, PCCP review expertise, sandboxes, and a commitment to balance premarket and postmarket evidence.
**What it means:** V regulated AI as a frozen model you validate once. VI plans for AI that keeps changing after clearance. If you\'re building an LLM-based device, this is the first commitment letter that acknowledges your product category exists.
MDUFA V printed p. 22 ("artificial intelligence or machine learning
(AI/ML)") vs. draft MDUFA VI p. 23 ("generative and agentic artificial
intelligence," PCCP reviews of AI-enabled devices).
### The caveat, and the takeaway
**This is a draft**. The commitment letter accompanies the MDUFA VI reauthorization, goals begin in FY2028, and FDA states explicitly that the recommendations remain subject to change until the final commitment letter publishes. Don\'t rebuild your regulatory strategy around it yet --- but do position for it.
**And you can still shape it.** The public comment docket (FDA-2026-N-6655 at regulations.gov) is open for 30 days from July 8, 2026, and FDA holds a hybrid public meeting on August 5 at White Oak (register by July 20). If the pre-sub fee --- or anything else in the draft --- affects your business, this is the statutory window in which FDA must consider and respond to comments.
The through-line across all seven changes: FDA is committing to be faster, more consistent, and more accountable. In exchange, it expects sponsors to show up with complete submissions, focused questions, and documented interactions. Teams that already operate that way will compound the advantage. Teams that don\'t have about eighteen months to build the habit.