
Background 🔗
On October 26th, 2023, FDA hosted a webinar to discuss three draft guidances that were issued earlier this year in an ongoing effort to modernize the 510(k) program:
- Best Practices for Selecting a Predicate Device to Support a Premarket Notification [510(k)] Submission
- Recommendations for the Use of Clinical Data in Premarket Notification [510(k)] Submissions
- Evidentiary Expectations for 510(k) Implant Devices
The FDA’s Center for Devices and Radiological Health (CDRH) frequently hosts webinars to discuss newly published guidance documents. These sessions provide stakeholders with insights and address their questions. To explore previous webinars, visit the FDA’s website.
Scope 🔗
This article provides a summary of the information described during the webinar (and in the corresponding FDA guidances) that are applicable to Software as Medical Devices. Thus, comments and guidance for implant devices will not be discussed in this article.
Efforts to Modernize the 510(k) Program 🔗
Since 2018, FDA has been making efforts to modernize the measures used to evaluate safety and effectiveness of new medical devices while continuing to create more efficient pathways to bring devices to patients. One of these propositions was to consider only predicates no older than 10 years. However, after receiving feedback from the public, it was determined that this might not be an optimal step forward. For example, for implant devices older predicates offer long-term safety and effectiveness data. Conversely, for software devices, newer predicates could be more indicative of modern safety features for cybersecurity and interoperability.
The purpose of the three draft guidances released on September 7th is to improve the predictability, consistency and transparency of the 510(k) program. At the same time, we’ve observed a trend where the Agency requests increasing information from new 510(k) applicants - new cybersecurity guidelines being a case in point.
Upon reviewing FDA’s guidance for “Best Practices for Selecting a Predicate Device to Support a Premarket Notification [510(k)] Submission”, it seems probable that we'll continue to see a surge in the volume of content in submissions. However, it’s important to note these are still draft guidances and are not yet finalized for implementation.
FDA Guidance: “Best Practices for Selecting a Predicate Device to Support a Premarket Notification [510(k)] Submission” 🔗
FDA’s guidance for “Best Practices for Selecting a Predicate Device to Support a Premarket Notification [510(k)] Submission” outlines recommendations for best practices for selecting a predicate device for your submission. This introduces a “hierarchical” method for evaluating potential predicates, which is explained below.
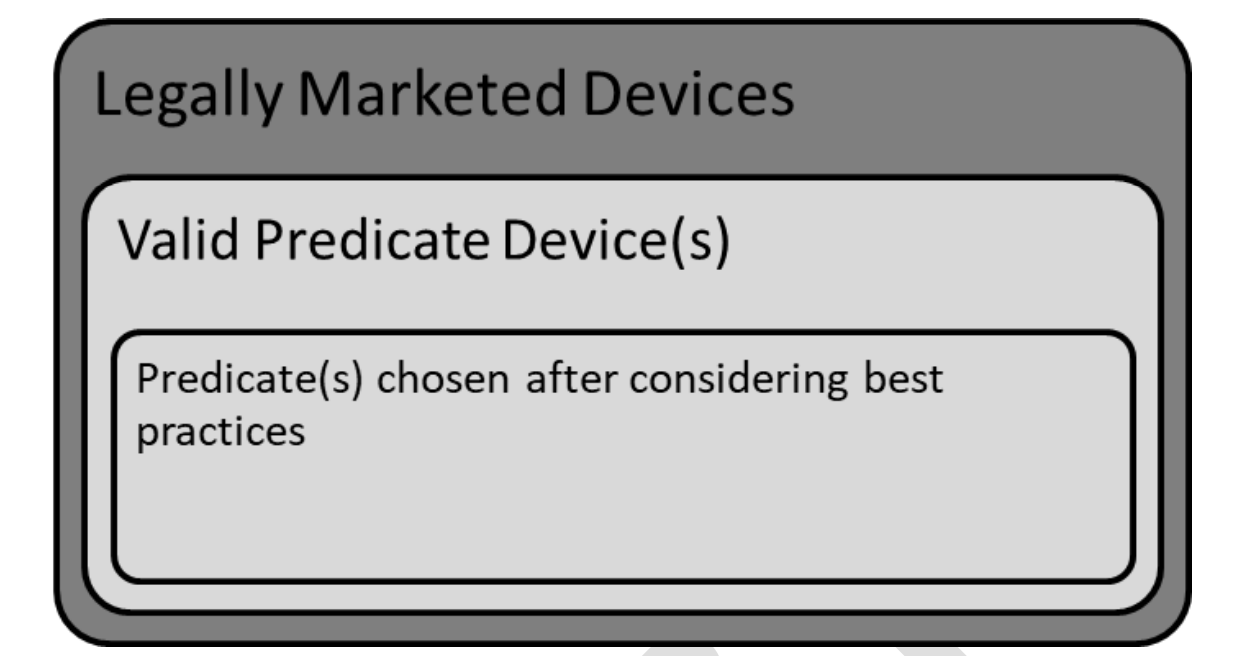
1 - Review Legally Marketed Devices 🔗
First consider the list of legally marketed devices.
A legally marketed device is a device that was legally marketed prior to May 28, 1976 (preamendments device), a device which has been reclassified from Class III to Class II or I, a device which has been 510(k)-cleared, or a device that was granted marketing authorization via the De Novo.
To review legally marketed devices, you will typically want to search the 510(k) and De Novo databases.
2 - Valid Predicate Devices 🔗
From the available legally marketed devices, consider which devices have the same intended use and similar technological characteristics. For any differences in technological characteristics, no new questions of safety and effectiveness should be raised.
Any legally marketed device that has the same intended use and similar technological characteristics is considered a “valid” predicate device.
3 - Chosen predicate device(s): 🔗
After reviewing steps 1 and 2 you might be thinking, "Isn't this what we already do?” But step 3 is where the new recommendations are introduced. Here, FDA suggests that we review all of the identified “valid” predicate devices and evaluate them using four (A-B) different parameters to determine which is the most suitable predicate device for our submission.
A - Consider valid predicate devices that use “well-established methods”
FDA recommends selecting a predicate device that has used “well-established methods”. This means reviewing your valid predicates’ 510(k) summaries and identifying those that cite FDA-recognized consensus standards, up-to-date FDA guidance documents (when appropriate), or widely acceptable testing methods that are supported published literature, among other examples.
This approach makes sense, and also facilitates you, the sponsor/applicant, in knowing exactly which standards to comply with or what test methods need to be followed.
B - Consider valid predicate devices that meet or exceed expected safety and performance
The Agency recommends selecting predicates that have a record of maintaining a safe and effective performance after commercial release. For this, recommendations include conducting a search for reported injury, deaths, or malfunctions using the following FDA databases:
- Manufacturer and User Facility Device Experience (MAUDE) Database;
- Medical Device Reporting (MDR) Database;
- MedSun Reports Database
This is a logical step and should naturally fit into your risk management strategy.
If, after reviewing these databases, adverse events or problems are noted in a valid predicate device, FDA recommends opting for a different valid predicate device. However, if this is not feasible, submitter should plan to mitigate (through design modifications, testing, etc.) that particular adverse event and describe it in the 510(k) submission.
C - Consider valid predicate devices without unmitigated use-related or design-related safety issues
Similar to the recommendation above, the FDA also recommends conducting a search of the Medical Device Safety and CBER Safety & Availability (Biologics) websites to assess whether any of the valid predicate devices have an associated use-related or design-related safety issue. Again, submitters should opt to select a valid predicate device without these issues.
D - Consider valid predicate devices without an associated design-related recall
Finally, the Agency recommends selecting a valid predicate device that has not been subject to a design-related recall. For this, you can review the Medical Device Recalls Database or Total Product Life Cycle Database to assess whether any of the valid predicate devices have an associated recall. Please note that not all recalls are design-related, and some can be manufacturing or labeling related.
Improving Transparency in 510(k) Summaries 🔗
The Agency recommends to incorporate this new step assessment into the 510(k) summary. Specifically, FDA recommends that submitters include a description of how the four best practices were used to choose the selected the predicate device. A tabular format like the one below is recommended.
| Valid Predicate Device | A - Well established methods | B – Meets or exceeds expected predicate performance |
C – Unmitigated use-related or design-related safety issues |
D – Associated design-related recall |
|---|---|---|---|---|
| 1 | Used internal methods that are not widely available and accepted |
High frequency of fractures reported in MDRs/MedSun reports |
Safety communication found on FDA’s website |
Design-related recall identified in FDA’s database |
| 2 | Used updated methods from current FDA guidance document |
Expected frequency of reported adverse events |
No known unmitigated use-related or design-related safety issues |
No design-related recall identified |
If a submitter can not find a valid predicate device that meets all four of the best practices, a rationale should be provided.
Furthermore, the FDA also recommends that the Performance Data section in the 510(k) Summary should also address how the submitter addressed any concerns that might have been identified when following best practice B.
FDA Guidance: “Recommendations for Use of Clinical Data in Premarket Notification [510(k)] Submissions” 🔗
It is widely understood that clinical data can sometimes be necessary to support a substantial equivalence determination in 510(k) submissions (about 10% of the submissions, as estimated by one of the FDA panelists during the webinar).
The Agency noted that clinical data is typically reviewed during decision point 5 in the flow chart in FDA’s Guidance “Evaluating Substantial Equivalence in Premarket Notifications [510(k)]”. This means that clinical data is often reviewed after reviewing the intended use, indications for use, and technical characteristics (decision points 1 through 4 in the flowchart).
However, clinical data may also be reviewed at decision point 2, to determine if new indications for use fall under the same intended use.
The FDA guidance discussed (“Recommendations for Use of Clinical Data in Premarket Notification [510(k)] Submissions”) describes four scenarios when clinical data may be necessary to determine substantial equivalence to a predicate device.
1 - Differences in Indications for Use 🔗
When indications for use differ between the subject and predicate device, it is important to determine whether these still fall under the same intended use. Indications for use are typically reviewed through the “Indications for Use” statement section in the eSTAR, device labeling (e.g., user manual), and clinical and/or scientific data. Some differences in indications for use that may require supporting clinical data include differences in patient population, target disease, anatomical site, among other examples.
2 - Differences in technological characteristics 🔗
Clinical data might be required when there are technological differences between devices. In the webinar, the FDA provided an example concerning an implantable device with an already approved range of sizes. If a manufacturer introduces sizes that fall within the previously cleared range, then non-clinical data might be adequate for determining substantial equivalence. However, if the new sizes set a new minimum or maximum, clinical data would likely be necessary. This is because introducing sizes beyond the established range demands evidence to ensure their safety, effectively broadening what's considered safe to use.
3 - Substantial equivalence cannot be determined with non-clinical testing 🔗
In certain scenarios, substantial equivalence cannot be established based solely on non-clinical tests. For example, if your predicate device conducted a clinical study, it's highly probable you'll need one as well. Some considerations include:
- The absence of a suitable model (like simulated bench tests or animal testing).
- Existing models might pose limitations to your device.
- A model might not accurately predict clinical outcomes.
- Specific questions related to anatomy or pathophysiology may need clinical evidence.
A clear example of this is devices intended to treat schizophrenia, given the limited non-clinical models available. Another instance could be a device designed to screen blood donors and their donations for transfusion-related infections. In such cases, standard analytical testing isn't sufficient to evaluate the risks of the blood supply associated with incorrect results.
4 - Newly identified risk for predicate suggest clinical data may be needed 🔗
As devices enter the market, new scientific insights about their safety can emerge, including newly identified or increased risks. This can influence the type and level of testing data required in to demonstrate safety and effectiveness. This is another reason why it is essential to review databases like MAUDE and TPLC during product design and development.
During the webinar, an attendee asked if a manufacturer who is currently conducting clinical data and discovers a new risk of a predicate device would need a different level of testing. The Agency responded that in this case, clinical testing is considered the “highest” level of testing, so the level of evidence would not be affected.
However, the FDA strongly suggested that in the case that a manufacturer becomes aware of a new or increase risk in a predicate device, a presubmission discussion should be scheduled as soon as possible.
When will final guidances be released? 🔗
An attendee posed this question during the webinar. In response, the Agency’s clarified that these draft guidances are not intended for immediate implementation. Comments may be submitted until December 6th, 2023. The FDA also shared that they follow a meticulous protocol for drafting and releasing guidance documents. Thus, once the comment period is closed, feedback will be reviewed and taken into consideration for the final guidance.
As of now, following the newly introduced predicate device selection methods will not be required in 510(k) submissions, but following best practices is recommended.
Conclusion 🔗
In conclusion, the FDA's recent guidance documents aim to demystify their evaluation process for 510k submissions, placing a strong emphasis on predicate selection and the integration of clinical data. This step-by-step approach to predicate selection speaks to the Agency's commitment to patient safety and device effectiveness. While these recommendations seem prudent and promising, they may present hurdles for some submitters, especially when a submitter’s ideal predicate doesn't perfectly align with the recommended best practices. However, in such situations, the FDA strongly encourages presubmission discussions.
