Most people read FDA guidance documents the way they read terms of service: skim, extract a few quotes, move on. This is a mistake. If you want to give actionable, correct, and instant advice on a live call, you need to read it the way a resident reads a clinical protocol: completely, repeatedly, and with deliberate memorization. At Innolitics we promise clients speed and certainty, and knowing the guidances cold (even better than FDA knows them) is a big part of that value proposition. There is nothing like being able to sway a reviewer’s opinion during a call by reciting a detail from a guidance document by memory. Here is the method.
The memory ladder 🔗
Everything below is organized around one idea: mastery sits on a five-rung ladder.
| Mastery Type | Human | AI Agent Analog |
|---|---|---|
| Rung 1. Verbatim recall. | you can reproduce the wording exactly, unprompted. | verbatim inside agent’s context window |
| Rung 2. Gist recall. | you can reproduce the substance in your own words, unprompted. | summary inside agent’s context window |
| Rung 3. Recognition. | you cannot reproduce it, but shown the item, you can say what it is and which category it belongs to. | compressed summary in context window, vector embedding based retrieval, supervised fine tuning |
| Rung 4. Known Unknown. | you remember only that the thing exists and what it is called, which is enough to know what to Google or ask ChatGPT. | retrieval keys or triggers in context window, vector embedding based retrieval, supervised fine tuning |
| Rung 5. Unknown Unknown. | either forgotten or never learned in the first place | Term appears after the foundation model weights training cutoff |
A concept at rung 5 is an unknown unknown, and those are what produce confidently wrong advice.
Synthesizing new documents from AI requires at least a recognition (rung 3) of mastery. Using AI to learn effectively requires a rung 4 level of mastery, so you know what question to even ask.
Step 1: Read it start to finish 🔗
Before anything else, read the entire document from start to finish. Every step that follows assumes you have seen the whole document at least once. This moves you up from rung 5.
Step 2: Extract every example and make flashcards 🔗
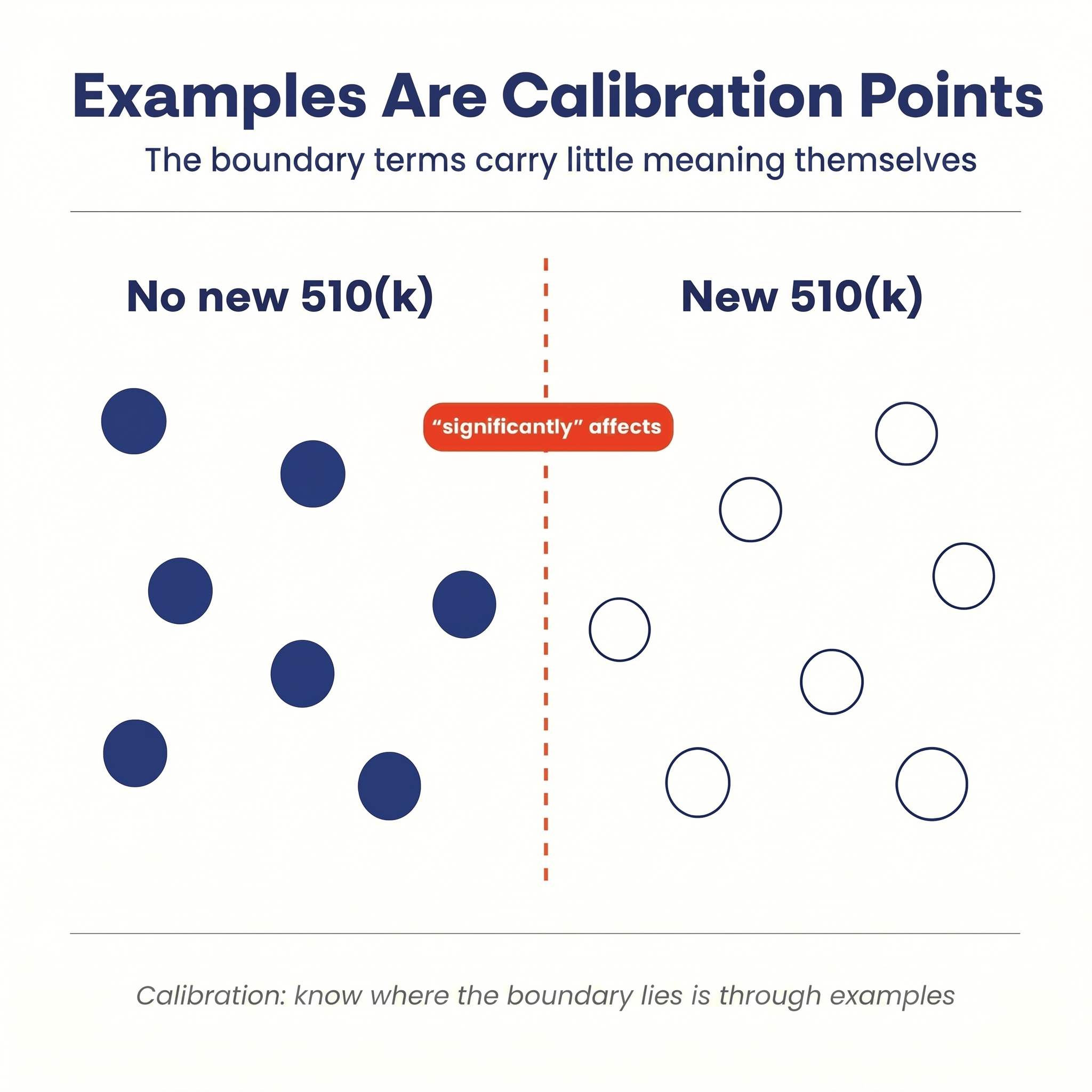
This is the step almost everyone skips, and it is the most important one. The stock text of a guidance is written in words like "significant," "low risk," and "can affect safety and performance." These words feel precise on first read but carry little practical value without examples. FDA knows this, which is why guidances include examples. They are not decoration; they are calibration points showing where the boundary actually sits. I call these “boundary terms”.
The vague language comes in two flavors. The first sounds absolute: "can affect safety and performance" reads like it covers everything, since almost any change can affect them. This absolutist interpretation is one of the most frequent cause of overly burdensome regulatory stance and costs companies millions of dollars and years of delays. There is in fact an implicit threshold below which a change is not “considered to affect safety and performance.” You estimate the threshold from FDA's examples, FDA enforcement letters, 510(k) and De Novo summaries, and refine it over years of client experience.
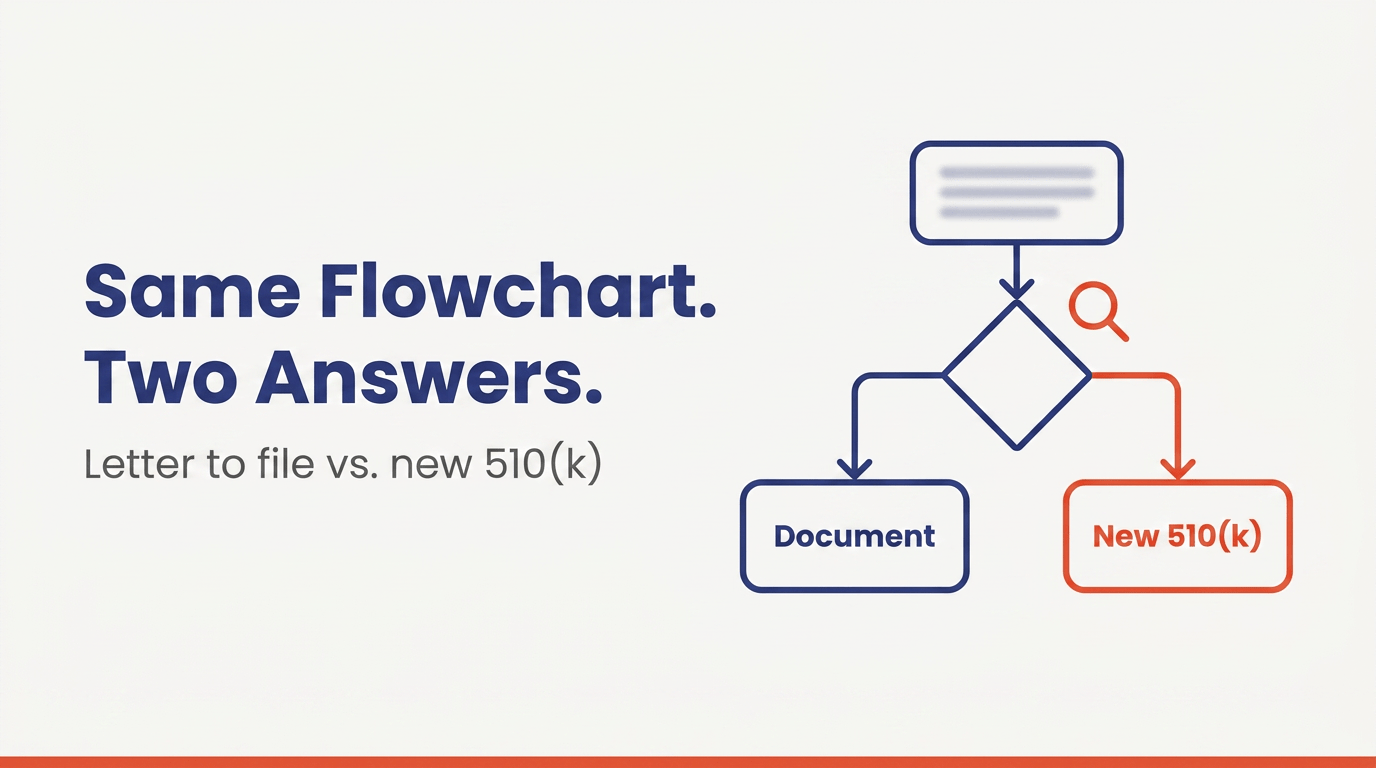
The second flavor is explicitly qualified: "significantly affects," "major change," "low risk." The qualifier admits a threshold exists but not where it is. The examples answer that too: when FDA lists six changes that require a new 510(k) and six that do not, it is handing you twelve calibration points on either side of the boundary. Extract every one onto a flashcard: the example on the front, the category and FDA's reasoning on the back. Old-fashioned paper flashcards are the best in my opinion since they give your brain more retrieval surfaces like spatial location, orientation, texture, even smell, but digital flashcards (like the Anki program) work too.
Step 3: Commit the key criteria to recall memory 🔗
Every major guidance has a small core framework that the rest of the document hangs on, and these frameworks must be committed to recall memory. The Clinical Decision Support guidance has its four criteria. The substantial equivalence decision runs on a short chain of questions: same intended use? same technological characteristics? if not, do the differences raise new questions of safety and effectiveness? The General Wellness guidance has its two-part test: general wellness intended use, and low risk. Each fits on an index card. Because a client call demands at least a faithful paraphrase, these need to be studied to the top two rungs.
Rung 1, verbatim recall, is reserved for the structure of the framework (the CDS guidance has four criteria, not "three or five") and the boundary terms: the phrases where FDA hangs meaning on the exact word, like "rely primarily," or "health care professional" rather than "user." This tier is small: perhaps fifty to a hundred words per guidance. A dedicated student can memorize about 200 words per day, so this is not an unreasonable ask, and the economic value of this knowledge is worth the effort.
Rung 2, gist recall, is the standard for the criteria themselves. You must recite them cold and unprompted, in your own words, without dropping a criterion, merging two into one, or softening a boundary term. Here is a passing rung 2 recitation of the CDS carve-out, the fifth of the Cures Act software exclusions. Software is not a device if it meets all four criteria:
- It does not acquire, process, or analyze a medical image or a signal from an IVD or signal acquisition system.
- It displays or analyzes medical information about a patient, or general medical information like guidelines and studies.
- It supports or provides recommendations to a health care professional.
- It lets that professional independently review the basis for the recommendation, so they are not relying primarily on the software for the clinical decision.
Notice, boundary terms like “acquire, process, or analyze”, “medical information”, “supports or provides”, "independently review the basis," and "rely primarily" are NOT paraphrased; they must be memorized verbatim in FDA’s words.
One more item belongs at the top rungs, and it is the easiest to skip: when NOT to use the guidance. Every guidance defines its own scope, usually up front, and deep mastery of a framework creates a pull to apply it everywhere. This is how experts miss the forest for the trees. You can recite all four CDS criteria flawlessly and still give wrong advice because the software is patient-facing, so the carve-out never applied in the first place. The 510(k) modifications guidance assumes a cleared device already exists. The General Wellness two-part test excludes anything invasive before the test even starts. Commit these scope boundaries to recitation memory alongside the criteria themselves, so the first question you answer on a live call is not "which criterion applies" but "does this guidance apply at all."
Scope traps are concrete, so learn them the same way you learn everything else: from examples. The CADe clinical performance assessment guidance is a classic. It reads like it covers every radiology CAD device that needs a clinical performance study, but the scope section excludes CADe intended for intra-operative use, and it excludes CADx, CADe/x, and CADa/o devices entirely (21 CFR 892.2060, 892.2090, and 892.2100). Recite that exclusion list cold, or you will spend a call calibrating a client against the wrong study design expectations.
| Guidance | Looks in scope | Actually out of scope |
|---|---|---|
| CADe Clinical Performance Assessment | Any radiology CAD device that needs a clinical performance study | CADe intended for intra-operative use; CADx, CADe/x, and CADa/o devices (21 CFR 892.2060, 892.2090, 892.2100) |
| Clinical Decision Support | Any software that offers diagnostic or treatment recommendations | Patient- and caregiver-facing software: the carve-out covers only recommendations to a health care professional |
| General Wellness | Any product with wellness claim wording | Anything invasive, implanted, or laser-based: the technology disqualifies it before the intended use test even starts |
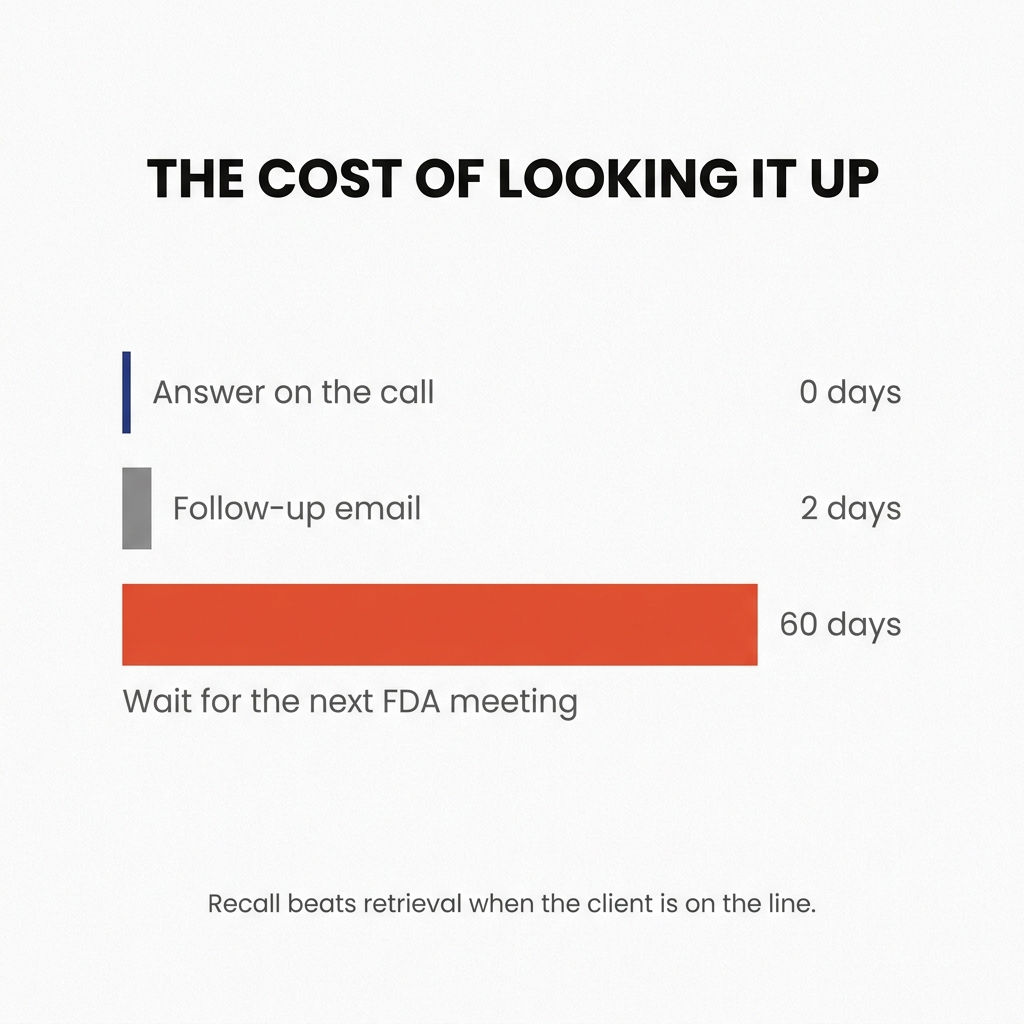
Why demand unprompted recall at all? Consultation happens in real time. When a client describes their product on a call, you walk them through the criteria as they talk, mapping their facts onto the framework live. "Let me look that up and get back to you" might seem inconsequential, but it results in a day or two delay at best and 60 days at worst to wait for another FDA meeting.
Step 4: Commit the examples to recognition memory 🔗
The examples get committed to recognition memory. You do not need to recite them, but if shown any similar example on a flashcard, you should be able to say which category it belongs to and, critically, why.
Why recognition and not recall memory? Because recognition better reflects how you will use this information in practice. You need to notice that the client scenario in front of you resembles an example and recall which side of the line it fell on. The "why" on the back of the card is what helps you generalize the recognition beyond the concrete example itself, because real scenarios never match an example exactly. You should also ask “why” in different ways so your brain can build richer representations and memory hooks that increase the likelihood that you’ll recall the right example at the right time. Once you have recalled the example, the rest of the relevant bits of the guidance, including recall memory items, pop into your working memory.
After much experimentation with AI memory systems, I have come to deeply appreciate the human brain’s ability to pattern-match instantly at multiple levels of abstraction. When an expert says, “You know that reminds me of…,” and nobody sees the relationship until the expert explains it, that is the kind of pattern-matching mastery that develops over time but can be accelerated by deliberately forming relationships during study. AI systems are unlikely to match this ability anytime soon due to computation, cost, and storage constraints. Currently, AI retrieval systems can only pattern-match at too shallow levels to be useful for high-stakes on-demand consulting engagements. Therefore, rapid representation formation, encoding, and retrieval, paired with critical thinking, will be a high-demand skill in the age of AI and should be mastered.
Below are some examples of what boundary terms and recognizable calibration examples look like:
| Boundary term | Guidance | One side of the line | Other side of the line |
|---|---|---|---|
| "rely primarily" | Clinical Decision Support | Device: time-critical sepsis alert — no time to independently review the basis | Non-device: guideline-based drug options with sources cited for the clinician to check |
| "acquire, process, or analyze a medical image or signal" | Clinical Decision Support | Device: software analyzes an ECG waveform to flag arrhythmia | Non-device: software uses already-reported lab values and demographics from the EHR |
| "could significantly affect the safety or effectiveness" | 510(k) modifications | New 510(k): new tissue-contacting implant material, or a new patient population | Document only: same-spec material from a new supplier, or a bug fix that leaves intended use unchanged |
| "low risk" | General Wellness | Not low risk: any implant, laser, or invasive technology, regardless of claim wording | Low risk: a sleep-tracking app suggesting relaxation, or a step-counting fitness tracker |
Step 5: Learn your organization's calibration 🔗
FDA's boundary is not the only one you need to internalize. Your own organization has its own calibration points, and they sit somewhere relative to FDA's: how it reads ambiguous cases, how much regulatory risk it will carry, where it draws the line between "document and proceed" and "go ask the agency." This position depends on the organization's culture, its philosophy, its business risk tolerance, its funding situation, and a host of other factors that no guidance document will tell you.
This calibration is usually learned the same way as FDA's: through examples rather than stated rules. You absorb it by working within the organization, through case studies, real client work, and other alignment training, watching how experienced colleagues call the cases that sit near the line.
Over time you will also develop your own calibration, distinct from both FDA's and your organization's. The key skill is to stay mobile in your thought: hold your calibration honestly, but update it based on the needs of the client in front of you.
The payoff: speed and certainty 🔗
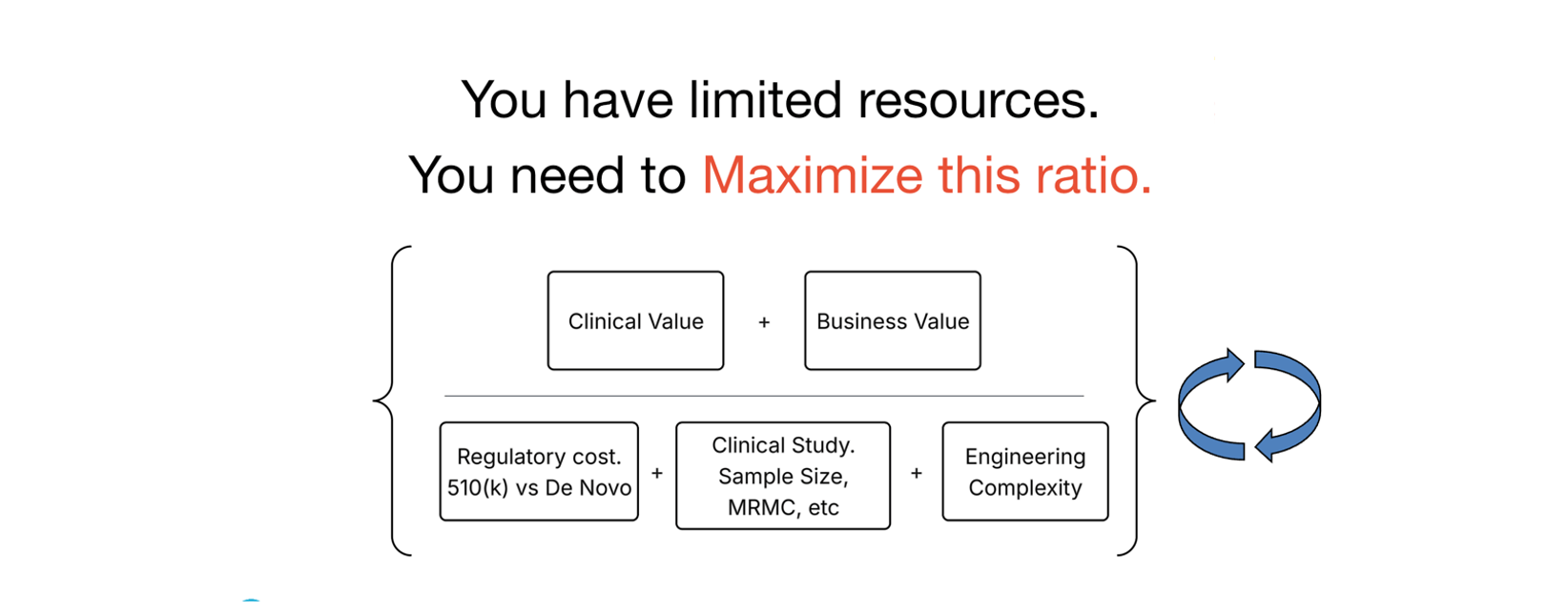
The goal is not memorization for its own sake. It is to build a high-value internal representation of the guidance, so you can play your part in the claims-to-cost maximization loop shown above. This is the core of the Innolitics value proposition. While other consultants need to phone a friend or, worse, request an unnecessary FDA presubmission meeting, we can provide an accurate answer instantly. And when the other experts in the room can do the same, a team of 5 can do in one meeting what would have taken a team 100x the size a year or more. That is the root of the speed and certainty promise and I am happy you are putting in the effort to learn it; patients deserve access to safe and effective devices and this is how we play our part.